Complicated heart surgery. What are heart surgeries? Narcosis or anesthesia
Heart valve replacement has been carried out everywhere for many years and has proven to be a safe and very effective operation to restore normal hemodynamics in the heart and the body as a whole.
Throughout life, valves are in constant operation, opening and closing billions of times. By old age, some wear of their tissues may occur, but its degree does not reach critical. Much more damage to the state of the valvular apparatus is caused by various diseases - atherosclerosis, rheumatic endocarditis, bacterial damage to the valves.
age-related changes in the aortic valve
Valvular lesions are most common among the elderly, the cause of which is atherosclerosis, accompanied by deposition of fat-protein masses in the valves, their compaction, calcification. The continuously recurrent nature of the pathology causes periods of exacerbations with damage to the valve tissues, microthrombosis, ulceration, which are replaced by remission and sclerosis. The proliferation of connective tissue ultimately leads to deformation, shortening, compaction and reduced mobility of the valve leaflets - a defect is formed.
Among young patients in need of artificial valve transplantation, mostly patients rheumatism. The infectious-inflammatory process on the valves is accompanied by ulceration, local thrombosis (warty endocarditis), necrosis of the connective tissue that forms the basis of the valve. As a result of irreversible sclerosis, the valve changes its anatomical configuration and becomes unable to perform its function.
Defects of the valvular apparatus of the heart lead to a total violation of hemodynamics in one or both circles of blood circulation at once. With the narrowing of these openings (stenosis), there is no complete emptying of the cavities of the heart, which are forced to work in an enhanced mode, hypertrophying, then depleting and expanding. In case of valve insufficiency, when its valves do not close completely, part of the blood returns in the opposite direction and also overloads the myocardium.
An increase in heart failure, stagnation in a large or small circle of blood flow provoke secondary changes in the internal organs, and are also dangerous for acute heart failure, therefore, if measures are not taken in time to normalize intracardiac blood flow, the patient will be doomed to death from decompensated heart failure.
The traditional valve replacement technique involves open access to the heart and its temporary shutdown from circulation. Today, more gentle, minimally invasive methods of surgical correction are widely used in cardiac surgery, which are less risky and as effective as open surgery.
Modern medicine offers not only alternative methods of operations, but also more modern designs of the valves themselves, and also guarantees their safety, durability and full compliance with the requirements of the patient's body.
Heart surgeries, no matter how they are performed, carry certain risks, are technically complex and require the participation of highly qualified cardiac surgeons working in a well-equipped operating room, so they are not performed just like that. With heart disease, for some time, the organ itself copes with the increased load, as its functional abilities are weakened, drug therapy is prescribed, and only if conservative measures are ineffective, the need for surgery arises. Indications for prosthetic heart valves are:
- Severe stenosis (narrowing) of the valve opening, which cannot be eliminated by simple dissection of the valves;
- Stenosis or insufficiency of the valve due to sclerosis, fibrosis, calcium salt deposits, ulceration, shortening of the valves, their wrinkling, limitation of mobility for the above reasons;
- Sclerosis of the tendon chords, disrupting the movement of the valves.
Thus, the reason for surgical correction is any irreversible structural change in the components of the valve, which makes the correct unidirectional blood flow impossible.
There are also contraindications for heart valve replacement surgery. Among them are the serious condition of the patient, the pathology of other internal organs, making the operation dangerous for the life of the patient, severe blood clotting disorders. An obstacle to surgical treatment may be the patient's refusal to operate, as well as the neglect of the defect, when intervention is inappropriate.
The mitral and aortic valves are most often replaced, they are also usually affected by atherosclerosis, rheumatism, and a bacterial inflammatory process.
Depending on the composition, the heart valve prosthesis is mechanical and biological. Mechanical valves made entirely of synthetic materials, they are metal structures with semicircular doors moving in one direction.
The advantages of mechanical valves are their strength, durability and wear resistance, the disadvantages are the need for lifelong anticoagulant therapy and the possibility of implantation only with open access to the heart.
biological valves consist of animal tissues - elements of the pericardium of a bull, valves of pigs, which are fixed on a synthetic ring that is installed in the place where the heart valve is attached. Animal tissues in the manufacture of biological prostheses are treated with special compounds that prevent immune rejection after implantation.
The advantages of a biological artificial valve are the possibility of implantation during endovascular intervention, the limitation of the period of taking anticoagulants within three months. Rapid wear is considered a significant drawback, especially if the mitral valve is replaced with such a prosthesis. On average, a biological valve works for about 12-15 years.
The aortic valve is easier to replace with any type of prosthesis than the mitral valve, therefore, when the mitral valve is damaged, different types of plasty (commissurotomy) are first resorted to, and only if they are ineffective or impossible, the possibility of a total valve replacement is decided.
Preparing for valve replacement surgery
Preparation for surgery begins with a thorough examination, including:
- General and biochemical blood tests;
- Urinalysis;
- Determination of blood clotting;
- electrocardiography;
- Ultrasound examination of the heart;
- Chest X-ray.
Depending on the accompanying changes, the list of diagnostic procedures may include coronary angiography, vascular ultrasound, and others. Mandatory consultations of narrow specialists, conclusions of a cardiologist and therapist.
On the eve of the operation, the patient talks with the surgeon, the anesthetist, takes a shower, dinner - no later than 8 hours before the start of the intervention. It is advisable to calm down and get enough sleep, many patients are helped by talking with the attending physician, clarifying all questions of interest, knowing the technique of the upcoming operation and getting to know the staff.
Technique for heart valve replacement surgery
Heart valve replacement can be performed through open access and in a minimally invasive way without incision of the sternum. Open operation performed under general anesthesia. After immersing the patient in anesthesia, the surgeon treats the operating field - the anterior surface of the chest, dissects the sternum in the longitudinal direction, opens the pericardial cavity, followed by manipulations on the heart.
prosthetic heart valve
To disconnect the organ from the blood flow, a heart-lung machine is used, which allows implanting valves on a non-working heart. In order to prevent hypoxic damage to the myocardium, it is treated with cold saline throughout the operation.
To install the prosthesis, the necessary cavity of the heart is opened using a longitudinal incision, the altered structures of its own valve are removed, an artificial valve is installed in its place, after which the myocardium is sutured. The heart is “started” with an electrical impulse or with direct massage, artificial circulation is turned off.
After the artificial heart valve is installed and the heart is sutured, the surgeon examines the cavity of the pericardium and pleura, removes blood and sutures the surgical wound in layers. To connect the halves of the sternum, metal brackets, wire, screws can be used. Ordinary sutures or cosmetic intradermal sutures with self-absorbable threads are applied to the skin.
Open surgery is very traumatic, so the operational risk is high, and postoperative recovery takes a long time.
endovascular aortic valve replacement
Endovascular technique valve replacement shows very good results, it does not require general anesthesia, so it is quite feasible for patients with severe comorbidities. The absence of a large incision allows you to minimize the stay in the hospital and subsequent rehabilitation. An important advantage of endovascular prosthetics is the possibility of performing surgery on a beating heart without the use of a heart-lung machine.
With endovascular prosthetics, a catheter with an implantable valve is inserted into the femoral vessels (artery or vein, depending on which cavity of the heart needs to be penetrated). After the destruction and removal of fragments of your own damaged valve, a prosthesis is installed in its place, which straightens itself thanks to a flexible stent-frame.
After installing the valve, stenting of the coronary vessels can also be performed. This possibility is very relevant for patients in whom both valves and vessels are affected by atherosclerosis, and in the process of one manipulation two problems can be solved at once.
The third option for prosthetics is from a mini-access. This method is also minimally invasive, but an incision of about 2-2.5 cm is made on the anterior chest wall in the projection of the apex of the heart, a catheter is inserted through it and the apex of the organ to the affected valve. Otherwise, the technique is similar to that for endovascular prosthetics.
Heart valve transplantation is in many cases an alternative to heart valve transplantation, which can significantly improve well-being and increase life expectancy. The choice of one of the listed methods of operation and the type of prosthesis depends both on the patient's condition and on the technical capabilities of the clinic.
Open surgery is the most dangerous, and endovascular technique is the most expensive, but, having significant advantages, it is the most preferable for both young and elderly patients. Even if there are no specialists and conditions for endovascular treatment in a particular city, but the patient has the financial opportunity to go to another clinic, then it should be used.
If aortic valve replacement is required, mini-access and endovascular surgery are preferred, while mitral valve replacement is more often performed by an open method due to its location inside the heart.
Postoperative period and rehabilitation
The operation to replace the heart valve is very painstaking and time-consuming, it lasts at least two hours. After its completion, the operated person is placed in the intensive care unit for further observation. After a day and with a favorable condition, the patient is transferred to a regular ward.
After an open operation, the sutures are processed daily, they are removed on the 7-10th day. All this period requires a stay in the hospital. With endovascular surgery, you can go home already for 3-4 days. Most patients note a rapid improvement in well-being, a surge of strength and energy, ease in performing ordinary household activities - eating, drinking, walking, showering, which previously provoked shortness of breath and severe fatigue.
If during prosthetics there was an incision in the sternum, then the pain can be felt for quite a long time - up to several weeks. With strong discomfort, you can take an analgesic, but if swelling, redness progresses in the area of \u200b\u200bthe seam, pathological discharge appears, then you should not hesitate to visit the doctor.
The rehabilitation period takes on average about six months, during which the patient regains strength, physical activity, gets used to taking certain medications (anticoagulants) and regular monitoring of blood clotting. It is strictly forbidden to cancel, independently prescribe or change the dosage of drugs; this should be done by a cardiologist or therapist.
Drug therapy after valve replacement includes:
- Anticoagulants (warfarin, clopidogrel) - for life with mechanical prostheses and up to three months with biological ones under constant coagulation monitoring (INR);
- Antibiotics for rheumatic malformations and the risk of infectious complications;
- Treatment of concomitant angina pectoris, arrhythmias, hypertension, etc. - beta-blockers, calcium antagonists, ACE inhibitors, diuretics (most of them are already well known to the patient, and he simply continues to take them).
Anticoagulants with an implanted mechanical valve make it possible to avoid thrombosis and embolism, which are provoked by a foreign body in the heart, but there is also a side effect of taking them - the risk of bleeding, stroke, therefore regular monitoring of INR (2.5-3.5) is an indispensable condition for life with a prosthesis.
Among the consequences of artificial heart valve transplantation, the most dangerous are thromboembolism, which is prevented by taking anticoagulants, as well as bacterial endocarditis - inflammation of the inner layer of the heart, when antibiotics are required.
At the rehabilitation stage, some disturbances in well-being are possible, which usually disappear after a few months - six months. These include depression and emotional lability, insomnia, temporary visual disturbances, discomfort in the chest and the area of the postoperative suture.
Life after the operation, subject to successful recovery, is no different from that of other people: the valve works well, the heart too, there are no signs of its insufficiency. However, the presence of a prosthesis in the heart will require changes in lifestyle, habits, regular visits to the cardiologist and control of hemostasis.
The first control examination by a cardiologist is carried out about a month after prosthetics. At the same time, blood and urine tests are taken, an ECG is taken. If the patient's condition is good, then in the future the doctor should be visited once a year, in other cases - more often, depending on the patient's condition. If you need to undergo other types of treatment or examinations, you should always warn in advance about the presence of a prosthetic valve.
Lifestyle after valve replacement requires giving up bad habits. First of all, you should stop smoking, and it is better to do this even before the operation. The diet does not dictate significant restrictions, but it is better to reduce the amount of salt and liquid consumed so as not to increase the load on the heart. In addition, the proportion of foods containing calcium should be reduced, as well as the amount of animal fats, fried foods, smoked meats in favor of vegetables, lean meats and fish.
High-quality rehabilitation after heart valve prosthetics is impossible without adequate physical activity. Exercise helps to increase overall tone and train the cardiovascular system. In the first weeks, do not be too zealous. It is better to start with feasible exercises that will serve as a prevention of complications without overloading the heart. Gradually, the volume of loads can be increased.
So that physical activity does not go to the detriment, experts recommend undergoing rehabilitation in sanatoriums, where exercise therapy instructors will help create an individual physical education program. If this is not possible, then all questions regarding sports activities will be clarified by a cardiologist at the place of residence.
The prognosis after transplantation of an artificial valve is favorable. Within a few weeks, the state of health is restored, and patients return to normal life and work. If the work activity is associated with intensive loads, then a transfer to lighter work may be required. In some cases, the patient receives a disability group, but it is not associated with the operation itself, but with the functioning of the heart as a whole and the ability to perform one or another type of activity.
Patient reviews after heart valve replacement surgery are more often positive. The duration of recovery is different for everyone, but most notice a positive trend already in the first six months, and relatives are grateful to surgeons for the opportunity to extend the life of a loved one. Relatively young patients feel good, some, according to the words, even forget about the presence of a prosthetic valve. Older people have a harder time, but they also notice a significant improvement.
Heart valve transplantation can be done free of charge, at the expense of the state. In this case, the patient is put on a waiting list, and preference is given to those who need an operation urgently or urgently. Paid treatment is also possible, but, of course, it is not cheap. The valve itself, depending on the design, composition and manufacturer, can cost up to one and a half thousand dollars, the operation - starting from 20 thousand rubles. It is difficult to determine the upper threshold for the cost of the operation: some clinics charge 150-400 thousand, in others the price of the entire treatment reaches one and a half million rubles.
Video: a new method for replacing heart valves
With certain cardiac pathologies, a person is recommended prompt elimination of the problem. For example, taking into account individual indications, a heart valve is replaced. Surgical correction (implantation, etc.) is widespread.
When is valve replacement scheduled?
It is indicated for symptoms suggestive of heart failure:
- the occurrence of shortness of breath;
- cardiac edema, pain;
- tachycardia;
- asthmatic manifestations.
If the effect of therapeutic treatment is insufficient, heart surgery is recommended to restore blood circulation.
The indications for it are:
- birth defects;
- defeat as a result of infection;
- lack of required density;
- violations in the valves (wrinkling, shortening, narrowing of the holes);
- the presence of scar tissue (fibrosis);
- inability to cut adhesions.
The operation is recognized as effective and safe.
aortic valve
This anatomical formation contributes to the cessation of the communication of the left ventricle (LV) with the aorta during the period of relaxation of the heart muscle (diastole). The leaflets of this valve close tightly during the impact of the blood stream, preventing its movement from the aorta back into the ventricle. Its area is normally 3-4 cm².
Congenital or acquired defects provoke a danger:
The combination of these factors causes heart defects.
Aortic heart disease
With deviations from the norm, aortic defects occur: combined, stenosis, insufficiency.
The valve leaflets are spliced to reduce the opening. The removal of blood from the ventricle is difficult.
- LV hypertrophy with the exclusion of arterial hypertension and a septal size of 15 mm or more;
- reduction of the hole area to 1 cm or less.
The pressure in the area between the aorta and the ventricle is more than 40 units.
Failure
The leaflets cannot close completely due to damage, and blood from the aorta is able to penetrate back into the ventricle.
Deficiency indicators for surgery:
- the volume of blood ejection into the aorta is less than 50%;
- the volume of reverse blood flow is more than 60 ml during the period of cardiac contraction;
- expansion of the cavity of the left ventricle up to 75 mm.
An open method of intervention with general anesthesia is practiced.
The combined defect arises as a result of a combination of a stenosis with insufficiency.
mitral valve
It is presented in the form of two valves between the atrium and the left ventricle. Blood flows from the first to the second. When the ventricle is compressed, the valve is closed. Blood at this moment is not pushed into the atrium, but through the aorta into the region of the vessels.
Replacing it with minimally invasive methods takes about three hours.. The open method is used in severe cases.
Correction methods
The endovascular method involves the introduction of a catheter with a prosthesis into the incisions of the femoral artery (or brachial) with local anesthesia. For dangerous defects, endovascular replacement is not applicable.
A minithoracotomy is a replacement of the mitral valve. In this case, a heart-lung machine is used. The chest is not completely opened, only a few incisions are made. Anesthesia is prescribed general.
Types of artificial valves
They differ in composition and method of manufacture.
Biological
The biological valve is made from natural tissues of pigs and other animals and is introduced for up to 15 years. After that, the replacement is repeated.
Advantages: no opening of the chest is required, the appointment of anticoagulants is provided only for 3 months.
Disadvantage: quick wear (12-15 years).
Mechanical
It is specially made using hypoallergenic materials such as plastic and metal. Such valves are installed indefinitely.
Advantages: durability, stability.
Disadvantages: obligatory provision of open access to the heart, lifelong anticoagulant therapy.
Donor valves are rarely practiced.
Features of preparation for surgery
In preparation for the operation, the following recommendations should be followed:
- Conduct appropriate diagnostics, which may include:
- echocardiography;
- laboratory tests of urine, blood (general and biochemical tests);
- chest x-ray;
- blood clotting test;
- Ultrasound of the heart.
- Take advantage of the advice of specialists who will be directly involved in the operational process:
- anesthetist;
- cardiologist;
- surgeon;
- specialist in respiratory therapy;
- middle medical staff.
- For 8 hours before the operation, completely refuse food. Before this, during the day, eat light food to avoid overloading the heart.
- Prepare psychologically, enlist the support of relatives.
Before the operation, you should rest, sleep. Take a shower no later than 8 hours before the intervention.
Priority for surgery and its cost
Prosthetic heart valves can be done free of charge, at the expense of the state. But for this you need to register in the queue. Benefits are available for emergencies.
Paid options are faster, but they are expensive.
The average cost of an implant is about one and a half thousand dollars, the operation itself is estimated from 70 to 400 thousand rubles, in some clinics and more.
Cardiac pathologies requiring surgical intervention are diseases subject to quotas. However, each clinic is issued by the Ministry of Health of the Russian Federation only a certain number of budget quotas, which are distributed by the commission.
Operation sequence
The operation to replace the heart valve begins after special preparation (breathing exercises, enema, etc.) and the introduction of anesthesia devices.
Difficulty in aortic valve replacement
Prosthetics of the aortic valve of the heart is carried out on an open organ. After opening the chest, the heart is connected to artificial blood flow. Without mandatory disclosure, the procedure is performed in a serious condition of the patient, unstable hemodynamics.
The methods of such surgical intervention provide access to the organ through the area of the femoral vein. The process is monitored on a special screen using vessel contrasting.
The biological material allows, after taking anticoagulants for a three-month period after the operation, to subsequently do without them.
Operation steps
After special preparation (it is described above) and the introduction of general anesthesia, surgical intervention involves the following steps:
- processing of the surgical field;
- longitudinal dissection of the sternum, opening of the pericardial cavity;
- connection of the artificial blood circulation mechanism;
- manipulations on the heart (removal of the affected valve);
- installation (implantation) of an artificial prosthesis;
- control of the functions of the implanted prosthesis, checking the seams;
- turning off artificial blood flow, "starting" the heart;
- suturing.
The procedure takes place under general anesthesia. Myocardial treatment throughout the operation (at least 2 hours) is performed with cold saline.
At the end of the process, the operated person is sent to the intensive care unit. He is not allowed to get up for two days. Initially, pain behind the sternum persists, high fatigue. On the fifth day, the patient can be discharged. Seams are processed daily. They are removed for 7-10 days.
Recovery after surgery
Modern valve implantation operations are performed with minimal risk. A person is discharged from the hospital on the fifth or sixth day, if there are no complications. However, the person undergoing this procedure must change their lifestyle.
Rehabilitation after surgery is important. The motor mode should be gentle:
- when planting, keep your legs at a right angle in the area of \u200b\u200bthe knees, do not cross them;
- before getting up from a chair, you should move to the edge;
- before getting out of bed, first roll onto your side;
- to lift objects from below, do not bend over, but sit down.
New movements should be added gradually, in a gentle mode. At first, the legs may swell, sleep and appetite may be disturbed, visual disturbances may occur.
Bouts of depression can be replaced by excessive cheerfulness. But these phenomena are temporary. Life after surgery quickly returns to normal.
With proper rehabilitation, after a few months (six months), the patient restores normal heart function and feels healthy.
It is important to undergo annual scheduled examinations, treatment, ensure proper dietary nutrition, and practice restorative physical education, which is important for breathing. For 2-4 weeks, you must follow the rehabilitation instructions prescribed by the doctor, control the fluid balance, and regularly monitor your health.
Annual surveys
They are shown to everyone who has gone through such an operation. Dispensary cardiological supervision includes:
- echocardiography (EchoCG);
- blood tests (clinical, biochemical);
- x-ray.
In addition, an INR test is performed monthly, reflecting the indicators of the blood coagulation system. During the consultation, the attending physician may prescribe medications, antibiotics, immunostimulants.
Foods and medicines rich in calcium are prohibited. In case of any deterioration in well-being, a doctor should be consulted without delay.
Diet after surgery
There are no strict restrictions in nutrition, but it is not recommended to abuse the intake of individual products.
- salt;
- coffee drinks;
- animal fats;
- carbohydrates.
- vegetable oils;
- fresh fruits and vegetables;
- fish.
In general, the diet is not strict, with standard recommendations. Alcohol consumption should be kept to a minimum. Smoking should also be limited.
Physical exercise
Activity in the post-rehabilitation period is practically unlimited. Only excessive loads and competitive sports should be excluded.
Consulting a doctor will help each individual in these matters. Recommended exercises, walking with increasing load, walking.
Physical activity has a positive effect on the state of blood vessels, the heart, strengthens the body as a whole. There are cases of returning to professional sports after surgery.
Complications and consequences of the operation
After surgical valve replacement, consequences and complications are possible. The most common are:
- instability of the surgical wound;
- migration of the implanted prosthesis;
- stroke, heart attack;
- complications due to prolonged immobility.
With any operation, there is a certain risk. To prevent thromboembolic complications and bleeding, anticoagulants with an individually selected dose are prescribed.
In any case, implanted prostheses are foreign bodies that can affect blood clotting and the formation of blood clots.
On the appointment of disability and forecasts
Non-working group II is determined for a period of one year after the completion of the operation to restore the myocardium. In the future, it is possible to transfer to group 3.
When establishing disability, cognitive deviations (reduction of mental abilities) are taken into account individually.
How long do they live with an artificial valve? The average life expectancy in this case is approximately 20 years. However, theoretically, the life of the valve is much longer (up to 300 years, according to doctors).
Contraindications for surgery
During surgery, there are always risks. Therefore, diseases of the internal organs can become an obstacle to the implementation of surgical intervention:
- severe heart disease;
- damage to the valve tissue of an infectious nature;
- thrombosis;
- exacerbation of rheumatism;
- complex valve deformity.
An obstacle may also be the patient's unwillingness, the neglect of the pathology. The main thing is to calculate the expediency and save life.
Heart valve surgeries are not uncommon these days. They are carried out regularly and successfully, thanks to the constant modernization of the process.
If the operation is performed out of time, there is a risk of developing pathologies due to the expansion of the left ventricle. This aggravates heart failure. With a quality operation, you will no longer have to experience pain. Forecasts are favorable. Only a scar will remind you of the transferred procedure.
Despite the fact that medical scientists are working to improve the technique of heart valve transplant surgery (biological and mechanical), and constantly create progressive versions of artificial valves, complications sometimes occur after heart valve replacement surgery.
Postoperative complications
Complications should not be confused with the process of wear of an artificial valve, which eventually becomes unusable. So, biological valves begin to function worse gradually, over 5–10 years, and mechanical valves can “work” without problems for 20–25 years, however, in this case, a person will have to constantly take anticoagulants (when transplanting biological valves, this is not required) .
Given the above trends, doctors recommend, in the process of treating heart disease, if necessary, that biological valves be transplanted to the elderly, for whom a ten-year valve life is acceptable, and besides, they do not have to drink additional drugs. Young patients are offered mechanical valves that do not fail for more than 20 years, although at the same time they have to prescribe drugs that prevent blood clotting .
Important: heart attack and stroke are the cause of almost 70% of all deaths in the world!
Hypertension and pressure surges caused by her in 89% of cases the patient is killed with a heart attack or stroke! Two-thirds of patients die in the first 5 years of the disease!
Death statistics during surgery
In people under 50 years of age, heart valve replacement surgery is usually uneventful, and the mortality rate does not exceed 1 percent. However, the older the patient, the higher the chance of dying during this heart surgery.
Mortality during heart valve replacement surgery:
Given the statistics and the fact that mechanical valves fail much less often, doctors decide which valve (biological or mechanical) to replace the “failed” patient's own heart valve.
A startling discovery in the treatment of hypertension
It has long been widely believed that It is impossible to get rid of HYPERTENSION permanently. To feel relief, you need to continuously drink expensive pharmaceuticals. Is it really? Let's figure it out!
Complications after surgery
Any heart surgery is a complex surgical procedure that can sometimes become complicated, causing unforeseen problems.
Growth of scar tissue - in some patients, at the site of valve replacement, there is a rapid growth of fibrous scar tissue. This can happen with both a seated biological valve and a transplanted mechanical valve. This complication leads to thrombosis of the artificial valve and will require repeated emergency surgery. However, after 2008, there was no report of this complication, that is, modern methods for carrying out the transplant procedure make it possible to avoid this scourge.
Bleeding as a result of taking anticoagulants - in the people, anticoagulants are called drugs that "thinn" the blood, but to be precise, these pharmacological agents do not make the blood more "fluid", they prevent the formation of blood clots, increasing the time of blood clotting. This property of anticoagulants makes it possible for blood, in any case, even if a clot begins to form in close proximity to the valve, to “wash it away” from the valve before it turns into a blood clot.
However, it happens that people who take anticoagulants for valve transplantation begin to suffer from bleeding in other organs of their body, and most often this is the stomach. Therefore, all patients are strongly advised to monitor the color of urine and feces (in case of bleeding, they darken) and contact your doctor for any signs of gastric distress.
Thromboembolism - a serious complication caused by valve thrombosis. The symptoms of thromboembolism are:
- dyspnea;
- dizziness;
- clouding of consciousness;
- loss of vision and hearing;
- numbness and weakness all over the body.
If at least one of the above symptoms occurs, the patient should immediately consult a doctor or call an ambulance.
Prosthetic valve infection - any, the most sterile foreign object placed inside a living body, can be subjected to infection. Therefore, if you have a fever, long-term respiratory problems (more than two days), or any infectious diseases, you should consult a doctor who, through tests and other tests (for example, MRI of the heart), will determine whether an infection of the artificial heart valve has occurred, or whether everything went well.
In order to avoid the development of infection of the implant, people with artificial valves, when visiting a dentist, as well as during procedures such as colonoscopy, gastroscopy, angiography, cardiac catheterization, etc., should inform doctors that they have an artificial heart valve. .
You should also be careful with skin infection from any accidental wounds, cuts, abrasions and blisters from shoes.
Hemolytic anemia - this complication occurs extremely rarely and is expressed in damage to a large number of red blood globules in contact with the implanted valve. Symptoms that hemolytic anemia has developed are:
- constant weakness;
- persistent fatigue and lethargy.
Although the symptoms of hemolytic anemia are similar to those of the body's reaction to taking anticoagulants, these complications have completely different mechanics of occurrence and development. Therefore, the patient should not figure out for himself what caused the ailment, but should immediately consult a doctor who, having made a diagnosis, will provide the correct treatment.
What valves to put (video)
The Russian industry produces many different products of the highest quality, which have no analogues in the world. Unfortunately, the same cannot be said for artificial heart valves.
Today, one of the best mechanical heart valves is Carbomedics Tophead. There are other excellent foreign analogues. Unfortunately, this cannot be said about Russian products - they are not so reliable, and they fail and quickly fail. Therefore, if we are talking about a young patient, it is better to pay more and put a European implant.
True, there is hope that soon, on the market of medical products, mechanical heart valves will appear that are not inferior and even superior in quality to foreign ones.
From this article you will learn: how the valve is replaced on the heart, who is assigned this operation. Possible complications, rehabilitation period. Life after such an operation.
Valves are structures that ensure the correct direction of blood flow. There are four valves in the human heart:
- Aortic.
- Pulmonary.
- Mitral.
- Tricuspid.
Due to various medical conditions, surgery may be required to replace one or more of them. The decision to perform a surgical intervention is made by a cardiologist, and a cardiac surgeon performs the operation. The patient is treated by the attending cardiologist.
Briefly about heart valves: what are they and why are they needed
All valves open during myocardial contraction and close during relaxation of the heart.
Valve arrangement
Structure and functions
When is valve replacement necessary?
The most common indications for replacing any of the valves are:
- insufficiency (when the valve does not close completely, and blood can flow in the opposite direction);
- stenosis (narrowing, due to which it is not able to open normally, and not enough blood moves in the right direction).
Most often, replacement of the aortic or mitral valve is required. Malformations of the tricuspid (tricuspid) usually appear in combination with defects of other valves. This requires the replacement of all valves affected by the disease.
The operation is performed with such a degree of valve damage, in which blood circulation is significantly impaired. The following symptoms appear:
- chest pain;
- fainting;
- dyspnea.
The doctor can also inform the patient about the need for surgery without severe symptoms, based on EchoCG data.
What are the indications for a heart ultrasound to replace a valve?
Another indication for valve replacement is infective endocarditis. With this disease, surgery is needed if:
- two weeks of antibiotic treatment had no effect;
- rapidly progressing heart failure;
- an intracardiac abscess appeared;
- blood clots form in the heart.
Contraindications
The operation cannot be performed with such pathologies:
- acute myocardial infarction;
- stroke;
- exacerbation of severe chronic diseases (diabetes mellitus, bronchial asthma, etc.).
Types of artificial valves, their features
They can be divided into two groups:
- Mechanical.
- Biological.
The latter are produced from animal tissues: the endocardium of pigs or the pericardium of calves.
For aortic valve defects, the Ross operation is popular, when a pulmonary valve is installed in place of the aortic valve (it is replaced with a biological prosthesis).
Advantages and disadvantages of biological prostheses:
Advantages and disadvantages of mechanical prostheses:
The feasibility of using different valves:
How is the operation performed
On the eve of surgery to replace the valve, the patient is prescribed sedatives.
12 hours before the manipulation you can not eat. Also stop taking any medications.
The operation itself is performed under general anesthesia. Lasts 3-6 hours. The operation is performed on an open heart using a heart-lung machine.
Carrying out heart surgery using a heart-lung machine
The operation is done in several stages:
- preparatory actions (introduction of the patient into deep sleep, preparation of the surgical field, etc.);
- incision and opening of the sternum;
- connecting the patient to a heart-lung machine;
- removal of the diseased valve;
- installation of a mechanical or biological prosthesis;
- disconnection from the heart-lung machine;
- closure of the sternum and suturing.
For the first 2-4 weeks after the operation, you will stay in the clinic in the hospital.
Postoperative period
For the first two days, the patient is prescribed bed rest. During this time, you may have:
- chest pain;
- visual disturbances;
- poor appetite;
- insomnia and drowsiness;
- leg swelling.
Tell your doctor if these signs occur, but don't panic—the symptoms usually go away within a few weeks.
Talk to your doctor about any changes in how you feel.
Possible Complications
The most dangerous complication is the occurrence of blood clots. The risk is higher with a mechanical prosthesis, especially in place of a mitral or tricuspid valve.
To prevent this complication, a constant intake of anticoagulants (Aspirin, Warfarin), as well as injections of Heparin in the postoperative period is necessary.
Infective endocarditis of the installed valve is in second place in terms of frequency of occurrence. The risk is increased with the installation of a biological prosthesis. Endocarditis can also occur during the installation of a mechanical prosthesis. In this case, microorganisms from adjacent tissues penetrate the synthetic material and become even more difficult to reach. This complication is very dangerous and often fatal.
- Chills.
- Fever.
- Violation of the established valve (again there are signs of heart failure).
Treatment of this complication involves antimicrobial therapy, and if it is ineffective, repeated surgical intervention.
To prevent endocarditis, all patients are prescribed antibiotics in the postoperative period.
The prognosis after such heart surgery is favorable. Surgery significantly reduces the risk of death from heart failure and improves quality of life.
Mortality after surgery is only 0.2%. The lethal outcome is mainly associated with thrombosis or endocarditis. Therefore, it is very important to take all the preventive drugs prescribed by the doctor.
Life after surgery
In the first year after valve replacement, you need to go to the doctor for a check-up every month. In the second year - once every six months. Thereafter, once a year.
During the examination, an ECG and EchoCG must be done.
Throughout life, you must follow these rules:
- Give up bad habits and drinking coffee.
- Take anticoagulants prescribed by your doctor.
- Follow a diet: give up fatty, fried, salty, eat more fruits, vegetables and dairy products.
- Work no more than 8 hours a day.
- Sleep at least 8 hours a day.
- Do not lead a sedentary lifestyle, walk more, spend at least 1-2 hours a day in the fresh air.
Physical exercise
Competitive sports and hard work are contraindicated.
It is possible and necessary to perform therapeutic exercises, agreed with the attending physician.
Precautions for future surgeries
Any surgical intervention, even dental, can provoke endocarditis. Therefore, be sure to inform the surgeon that you have undergone heart valve replacement surgery.
To prevent an inflammatory process in the heart, you need to take an antibiotic 30-60 minutes before the surgical procedure. It can be Amoxicillin, Azithromycin, Ampicillin or Cephalexin to choose from. Check this with your doctor first.
Hello! Last year, in October, I was diagnosed with heart disease. Tricuspid insufficiency of the heart valve, and pulmonary hypertension, besides, Raynaud's syndrome. They said for an operation, I went through all the medical examinations and tests. A few days later, I I was supposed to be sent for an operation. But I refused in the last minutes, I was very scared, I don’t know what will happen next. I also have a goiter. What should I do, please tell me, I am completely at a loss.
Hello, Natalia. If your local doctors suggest you have surgery, you need to decide, because over the years complications come, not improvements. But it's up to you to decide.
Good afternoon Please tell us how to be! The husband is a dynamic patient for 5 years. In 2013, I was diagnosed with infection, endocorditis. I sent documents for valve replacement to the Novosibirsk clinic, but they refused. Now he is in the hospital, there was pulmonary edema. At present, the edema has been eliminated, he was transferred from the intensive care unit to the rheumatology department. There, the Doctor said that “edema is the beginning of the end”, that they can’t help and will be discharged. What should we do? HELP SAVE YOUR HUSBAND. Where can we turn for help?
Hello Veronica. I really sympathize with you, but our site does not keep links with any clinics. You need to search.
It has been 5 months since mitral and aortic valve replacement surgery. He had a long fever and cough, and there was congestion in his lungs and liver. After taking antibiotics for a long time, she coped with these problems. Now, against the background of not feeling bad, there are days when severe shortness of breath appears. Myrcative arrhythmia did not go away. I accept: nebivolol, tlrosemide, lazortan and xarelto. Bio valves. Age 60 years. Periodically, a burning sensation appears in the whole body, or as if under a current. What to do? Thank you.
Lussy, our site does not prescribe treatment, this is unacceptable via the Internet. Based on your comment, an additional face-to-face consultation with a cardiologist is needed regarding the adjustment of the medications taken.
Hello. My mom had heart surgery to replace her mitral valve with an artificial one. The operation was February 8, 2018. And the other day, she started to get really pissed off. What could it be?
Hello Nastya. This may be a circulatory disorder, vasospasm, increased pressure, etc. you need to contact your doctor.
Hello, in 2004 Tetrado fallo was operated on. Now there is insufficiency of the pulmonary valve (I don’t have it, there is a mono-cusp) operation is recommended. I’m very afraid, I have two small children. They said the risk of the operation is very high, I don’t know what to do and how much I can do without it? How dangerous is this operation?
Olga, if they offer help, you need to decide. Any operation is a risk. However, no one can accurately judge the outcome in advance. I wish you more optimism and everything will be fine!
Hello, I had an operation, I changed the valve. Thank you for your support too!
Hello Olga. We are very glad that you dared and changed your life for the better.
There are a lot of reasons for the development of intercostal neuralgia, these are: degenerative processes in the spinal column, especially in chronic or acute form, constant worries and stresses, poisoning of the body with various toxins or chemicals, an acute shortage of vitamin B, which in many cases occurs due to intestinal inability suck it up, etc. others
To eliminate neuralgia, you need to know the exact cause. Eliminates pain with antispasmodic and sedative. For example, spazmolgon plus phytosed.
Try drinking a decoction of several herbs: chamomile and lemon balm. They need to be taken in equal parts, pour boiling water and boil in a water bath for 15 minutes. Next, add a teaspoon of honey. Consume 2 times a day.
Good afternoon, my mother underwent mitral valve prosthetics with a mechanical valve, tricuspid valve plasty. The area of the left atrioventricular orifice was 1.2 cm2, SV = 65. She had restenosis. For the first time in 2007, a closed commissurotomy was performed. As the surgeons said after the operation. She had a big heart (there was hypertrophy). She was operated on, she spoke normally, walked. Then, after 2 days, according to the doctors, her heart stopped, because of this, cerebral edema developed. She was immediately transferred to intensive care. Dad and I are not allowed into intensive care. Doctors say his condition is stable. Tell me please. What could cause cardiac arrest and cerebral edema? I am very worried about her, she is my life, my everything. ((((((((.
Hello Faridun. There can be many reasons for cardiac arrest and the development of cerebral edema, for example, a sharp violation of blood circulation. It is impossible to state such facts with certainty. You need to believe and hope that everything will work out.
The doctor replaced my mitral and aortic valves. The question in nutrition is whether spices can be eaten.
I was urgently shown an operation to replace the valve, for a year now I have been living without it, I am afraid and I have a job 12 in 12 will I be able to work? And how is the postoperative period?
Hello Victoria. You have to choose between work or health. With heart disease, work for 12 hours is contraindicated. You can't delay the operation. If the valve stops functioning properly, then the person develops heart failure. At the same time, the cardiac muscle wears out, blood stasis forms in all internal organs. As a result: the human body is depleted. Over time, these complications lead to death. Much depends on the professionalism of surgeons and the specific method of installing the prosthesis. The total time of the patient's stay in the cardiac surgery center: from 2 weeks to 1.5 months.
Be healthy!
My husband underwent heart surgery on January 31 to replace the methal valve with an artificial one. Discharged after 5 days with fever. The temperature is right now. They prescribed a drug for the temperature of the suppository Diclofenac or voltaren.
When you make candles, the temperature disappears. When will it be ok?
Maybe instead of Warfarin something better and inexpensive is needed. This drug gives a complication on the stomach. In short, they cut everyone out, but we are not doctors, I don’t know how to care.
The most difficult thing is that the pressure is low. At first it was 80/57, now it's 100/60 and there is an arrhythmia.
Help, plz.
I was in the hospital in (Sklifa)
Lyudmila, Ivanovna, blood pressure can decrease by removing the obstruction to normal blood flow (after mitral valve replacement), which should stabilize over time. In addition, patients after prosthetics receive a lot of drugs, and it is possible that among them there are also those that reduce blood pressure. Check all the drugs that have been prescribed, and if there is an antihypertensive, reduce its intake by 2 times. And for the causes of high body temperature after valve replacement surgery, there can be a lot. Most often it is infective endocarditis, the addition of a respiratory infection (pleurisy, pneumonia, acute respiratory viral infections, etc.), exacerbation of any chronic inflammatory process that exists before surgery. It is important to establish the cause. If the patient was examined by a specialist, the drugs were prescribed, do not change the medicines yourself, just try to give them to your husband after eating, then the effect of irritation of the mucous membrane will be the least.
Be healthy.
Thank you very clearly written in simple words
In contact with
The operation on the heart, which at one time was compared with the first manned flight into space, is exactly 50 years old. It is very pleasant that our surgeon Vasily Kolesov conceived and executed it. Now it is one of the most common procedures in the world to prevent a heart attack and bears the name of its developer.
"The Soviet surgeon dared to raise his hand on his heart" - in 1964 this news outraged the entire world medical community. No one believed that coronary heart disease could be treated with surgery. Numerous experiments on animals ended unsuccessfully. But Vasily Ivanovich Kolesov, a professor at the Leningrad Medical University, proves that operating on a healthy heart in dogs and a diseased heart in humans is not the same thing, and he decides on a bold experiment.
Stanislav Pudyakov then assisted the surgeon. He recalls: a 44-year-old patient was tormented by severe pain in the region of the heart.
“His idea, if compared historically, is similar to the thoughts of Tsiolkovsky, who said that tomorrow we will be on the moon. They didn’t believe him until they really flew. And until Vasily Ivanovich did this first operation, no one believed in it” - says Stanislav Pudyakov.
The surgeon operated on a beating heart, which was also hard to believe. No one had done this before Kolesov, neither in our country nor in the world. Moreover, the doctor literally felt the sore spot with his hands. The equipment for diagnosing heart diseases simply did not exist then.
To restore the normal blood supply to the heart, Kolesov singled out the internal thoracic artery and sewed it to the coronary artery below the narrowing caused by the so-called atherosclerotic plaque. The blood flow went around, the patient was saved from a heart attack.
After the operation, people quickly returned to normal life and forgot about the pills forever. About operations that saved people from heart attacks and pains in the heart, they started talking abroad as a sensation. American magazines wrote about Kolesov: "Pioneer of coronary surgery."
“There were confessions among colleagues, among foreigners. A lot of Americans, Germans, French came, they looked at these operations with great curiosity and really wanted to continue what was started here,” says surgeon Alexander Nemkov.
Vasily Kolesov immediately warned: it would not be easy for young surgeons to repeat this. From now on, operations must be performed on a stopped heart. The advice was regarded as a guide to action. In 1967, American surgeons put them on stream.
The method of treatment of coronary heart disease, proposed by Vasily Ivanovich Kolesov, is considered the most effective after 50 years. Operations are performed by the best cardiac surgeons in clinics around the world. This is aerobatics, because, in fact, doctors must restart the main human organ.
“Speaking specifically about the operation of Vasily Ivanovich Kolesov, it is now being performed widely on a beating heart. What he did is incredible. The range of suture material that we use has changed, the needle holders that we use have changed incredibly. We use special magnifying lenses and we see this artery magnificently, which can be a millimeter, a millimeter and a half,” says surgeon Leo Bokeria.
Like half a century ago, coronary heart disease is the most common disease in the world. Now we can say with confidence that doctors have learned to deal with it. Thanks to the revolutionary method of Vasily Kolesov, even the most difficult patients can be saved.
May God grant everyone to live a long life so that the surgeon's scalpel never touches his heart. However, not always cardiac surgery can be replaced by therapy.
When is surgery necessary?
- When conservative therapy does not give the desired result.
- When, despite all the ongoing treatment, the patient's condition continues to deteriorate.
- When there are severe congenital heart defects, severe arrhythmia, cardiomyopathy.
By urgency, cardiosurgical operations are emergency and planned.
- Emergencies are carried out when a person's life is in serious danger. This happens when a myocardial infarction occurs, a blood clot suddenly breaks off, or aortic dissection begins. They do not tolerate delay in surgery when the heart is injured. The consequences of delay are severe.
- Planned are carried out in accordance with the developed plan for the correction of the patient's health. The date of the operation may be postponed depending on the circumstances. For example: with a cold, to avoid additional stress on the heart, or when the pressure suddenly dropped.
Surgical intervention differs in the technique of execution. There are such types of heart operations:
- with the opening of the chest;
- without opening the chest.
Chest opening operations
Such surgical intervention is used in especially severe cases, when full accessibility of the heart is required during the operation.
Opening of the chest is performed with such pathologies:
- tetralogy of Fallot (the so-called congenital heart disease with four serious violations of the anatomical structure);
- serious anomalies of intracardiac partitions, valves, aorta and coronary arteries;
- heart tumors.
The patient arrives at the hospital one day before the operation. Passes inspection, gives written consent. Be sure to wash with antibacterial soap and shave your hair. Where do you shave your body hair? The hair will be shaved at the site of the proposed incision. If you are going to have a coronary bypass surgery, you will have to shave your legs and groin. In the case of a heart valve replacement, it is necessary to shave the hair in the lower abdomen and in the groin area.
The surgery is performed under general anesthesia. To gain access to the heart, the surgeon opens the chest of the person being operated on. The patient is connected to an artificial lung ventilation apparatus, the heart stops for a while and surgical manipulations are performed with the organ.
How long the operation takes depends on the severity of the pathology. On average, several hours.
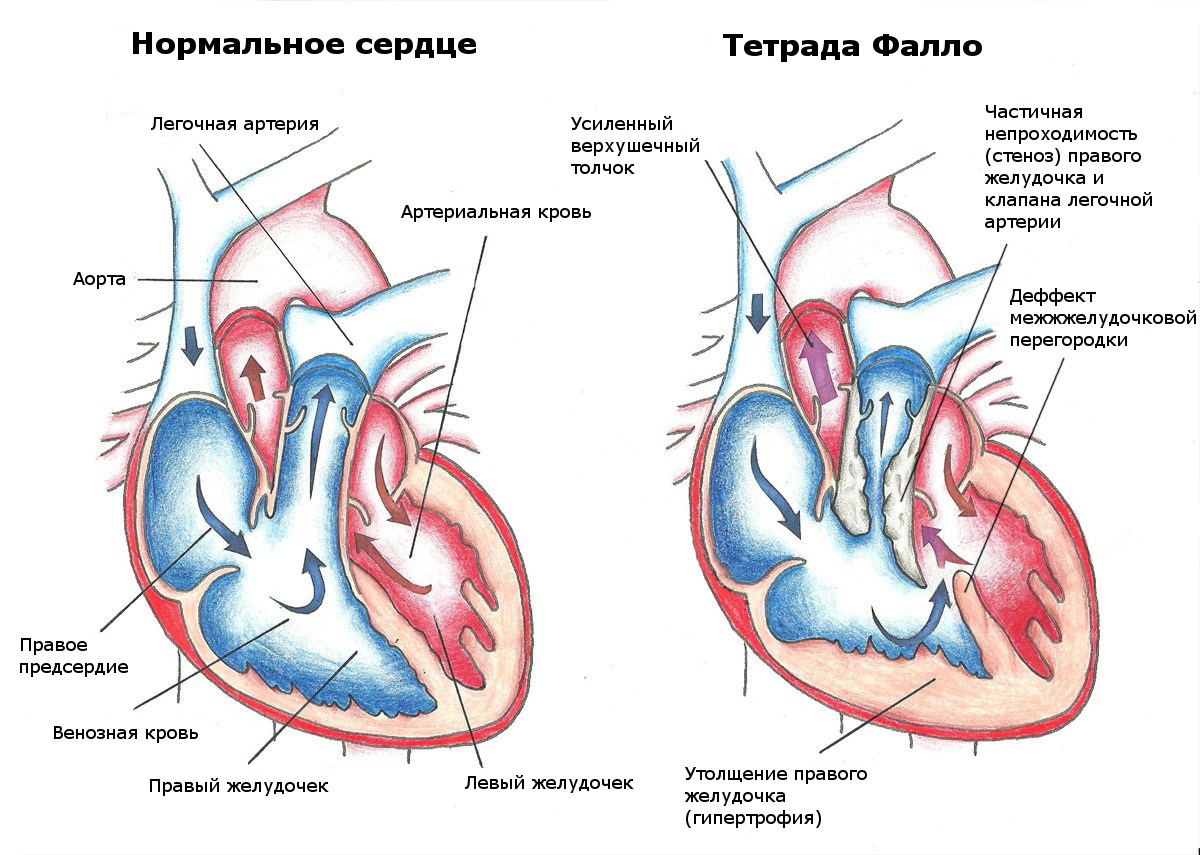 Tetralogy of Fallot
Tetralogy of Fallot Open heart surgery has two advantages.
- The surgeon has full access to the patient's heart.
- Such a surgical intervention is possible without state-of-the-art medical equipment.
However, there are also significant drawbacks.
- Surgical manipulations with the heart last several hours, which leads to fatigue of the operating team, during the operation there is a higher probability of making an erroneous action.
- Opening the chest is fraught with various injuries.
- There is a noticeable scar after heart surgery.
- Various complications are not excluded:
- myocardial infarction,
- thromboembolism,
- bleeding,
- infections;
- coma after surgery.
- A long recovery is required with significant limitations in the patient's activities.
In most cases, when surgery is performed with an opening of the chest, disability is given after heart surgery, as after a heart attack.
What operations and under what pathologies are performed on the open heart?
Pathologies of the coronary arteries
Coronary artery bypass grafting is done in case of serious atherosclerotic lesions of the coronary arteries, which led to a severe form of coronary heart disease. The essence of shunting is to create a bypass for blood flow to the heart using a shunt, for which an artery or vein taken from the patient is used. For example: mammary coronary artery bypass grafting (MCB) is performed using the internal mammary (mammary) artery.
 Operation Ross
Operation Ross Heart valve defects
Today, valves made from the patient's biological material are used to replace damaged valves.
- The Ross procedure involves using the patient's own valvular pulmonary artery to replace a diseased aortic valve. An implant is placed in place of the pulmonary valve. Eliminates complications associated with rejection of a valve made of foreign material. Made for both adults and children.
- The Ozaki operation involves the use of the patient's own tissue. Only in this case, the replacement of the aortic valve is performed with a valve made from the patient's pericardium. Complications with valve rejection are not observed for the same reason.
But now, the diagnosis has been made and the doctors understand what needs to be done next. I would like you to understand well by this moment, what will be discussed when they will explain everything in detail to you, what was found during the examination, what diagnosis was made, what needs to be done and when to choose the best way of treatment.
Here and now the main questions are being decided, and you must exactly imagine what you want to know before you make a decision on which a lot depends.
There are several options for conversation.
- You will be offered operation, as the only way out, and doctors believe that it needs to be done urgently.
- You are offered an operation, but they say that it can be postponed for a while.
- You are denied an operation for a variety of reasons.
You need to understand what is being said and prepare for the conversation. Try to be calm and confident in yourself and in the doctors who want to help you. You must be together, on the same side, in the fight for the future of the child. Discuss everything, but your questions should be literate. Believe me, a lot depends on this too.
What do you need to know about in order to ask the right question? What are the operations? What should the child do? How will it all be? Who will do it? Let's talk about it calmly.
Today, all interventions, or operations, for congenital heart defects can be divided into three categories: "closed" operations, "open" and "X-ray surgery".
✔ Closed Operations These are surgical interventions in which the heart itself is not affected. They are performed outside of it, and therefore do not require the use of any special equipment other than conventional surgical instruments. The cavities of the heart are not “opened” with them, which is why they are called “closed”, and they are widely performed as the first stage of surgical intervention.
✔ Open Operations- These are surgical interventions in which it is necessary to open the cavities of the heart in order to eliminate the existing defect. For this, a special apparatus is used - a heart-lung machine (AIC), or "heart-lungs". For the period of the operation, both the heart and the lungs are switched off from the circulation, and the surgeon gets the opportunity to perform any operation on the so-called "dry", stopped heart.
All the patient's venous blood is sent to the apparatus, where, passing through an oxygenator (artificial lung), it is saturated with oxygen and gives off carbon dioxide, turning into arterial. Then the arterial blood is pumped into the patient's aorta by a pump, i.e. into the systemic circulation. Modern technologies allow all the internal parts of the device (including the oxygenator), with which the patient's blood comes into contact, to be made "disposable", i.e. use them only once and only for one patient. This dramatically reduces the number of possible complications.
Today, thanks to AIC, it is possible without much risk to turn off the heart and lungs from work for several hours (and the surgeon has the opportunity to operate on the most complex defects).
✔ X-ray surgery appeared relatively recently, but, thanks to the incredible progress of modern technologies, they have already taken their rightful place in the arsenal of cardiac surgery. More and more doctors are now using thin catheters, the ends of which are fitted with balloons, patches, or expandable tubes (folded like a folding umbrella). With the help of a catheter, these devices are carried into the cavity of the heart, or into the lumen of the vessel, and then, expanding the balloon, break the narrowed valve with pressure, increase or create a defect in the septum, or, conversely, by opening the patch umbrella, this defect is closed. The tubes are inserted into the lumen of the desired vessel and create a wider lumen. In adults, they even try to pass an artificial aortic valve through the catheter in this way, but so far these are only attempts. Doctors monitor the course of an X-ray surgical operation on the monitor screen and clearly control all manipulations with the probe, and therefore the advantage of such operations is not only less trauma, but also high safety and efficiency. X-ray surgery has not yet supplanted traditional surgical methods, but it is gaining more and more space both as an independent method and as an “auxiliary”, i.e. which can be applied not instead of, but together with the usual operation, sometimes simplifying and supplementing it in many ways.
Depending on the type of defect and the condition of the child, surgical operations can be emergency, urgent and elective, i.e. planned.
emergency heart surgery are the ones that should be done immediately after the diagnosis is made, because any delay threatens the life of the child. With congenital malformations, such situations are not uncommon, especially when it comes to newborns. Here the question of life is often decided by hours and minutes.
Emergency operations- those for whom there is no such insane urgency. The operation does not need to be done right now, but you can calmly wait a few days, prepare both you and the child, but it must be done urgently, because then it may be too late.
Planned, or elective, operation- this is an intervention made at the time chosen by you and the surgeons, when the child's condition does not inspire fear, but the operation, nevertheless, should not be postponed.
No cardiac surgeon will ever suggest surgery if it can be avoided. So, anyway, it should be.
Depending on the approach to surgical treatment, radical and palliative operations are distinguished.
✔ Radical heart surgery is a correction that completely eliminates the defect. It can be done with an open ductus arteriosus, septal defects, complete transposition of the main vessels, abnormal pulmonary vein drainage, atrioventricular communication, Fallot's tetrad and some other defects, in which the heart is fully formed, and the surgeon has the opportunity to completely separate the circulatory circles, while maintaining normal anatomical relationships. Those. the atria will connect to their ventricles through correctly positioned valves, and the corresponding great vessels will depart from the ventricles.
✔ Palliative heart surgery- auxiliary, “facilitating”, aimed at normalizing or improving blood circulation and preparing the vascular bed for radical correction. Palliative operations do not eliminate the disease itself, but significantly improve the child's condition. With some very complex defects, which until recently were generally inoperable, the child will have one, and sometimes two palliative operations, before the final radical stage becomes possible.
During a palliative operation, another "defect" is surgically created, which the child does not initially have, but due to which the circulatory pathways disturbed by the defect in the large and small circles are changed. These include surgical expansion of the atrial septal defect, all variants of intervascular anastomoses - i.e. additional shunts, messages between circles. The Fontan operation is the most “radical” of all such methods, after which a person lives without a right ventricle at all. With some of the most complex heart defects, it is impossible to correct the anatomically, and surgical treatment aimed at correcting blood flow can be called the “final” palliative correction, but by no means a radical operation.
In other words, with heart defects, when the intracardiac anatomy - the structure of the ventricles, the condition of the atrioventricular valves, the location of the aorta and the pulmonary trunk - are so changed that they do not allow for a real radical correction, today's surgery follows the path of eliminating poorly compatible with life of circulatory disorders, and then - long-term palliation. The first stage of this path is saving lives and preparing for further treatment, and protection from future complications, the second is the final stage of treatment. All together - this is a long way to the final operation, and on it one, two, and sometimes three steps must be overcome, but, ultimately, to make the child healthy enough for him to develop, learn, lead a normal life, which this long-term palliation will provide him. Check it out, not so long ago - 20-25 years ago it was simply impossible, and children born with the defects of this group were doomed to death.
Such a “final palliation” is the only way out in many cases; although it does not correct the defect itself, it provides the child with an almost normal life by improving the mixing of arterial and venous blood flows, the complete separation of circles, and the elimination of obstructions to blood flow.
Obviously, the very concept of radical and palliative treatment for some complex congenital heart defects is largely arbitrary, and the boundaries are erased.
Cardiovascular diseases, unfortunately, occupy one of the first places in terms of mortality in our country. But cardiology does not stand still, but is constantly being improved. In this area, new methods of treatment are constantly emerging and the most modern technologies are being introduced. Naturally, people suffering from severe heart diseases are interested in all the innovations in cardiology, and therefore in various methods of surgical interventions.
When is Cardiac Surgery Used?
Absolutely not any violation in the work of cardiac activity entails surgical intervention. There are absolutely clear criteria on which the attending physician relies, recommending this or that cardiological operation. Such indications may be:
- Significant and rapidly progressive deterioration of the patient's condition associated with chronic heart failure.
- Acute conditions that threaten the life of the patient.
- Extremely low efficiency of simple drug treatment with clear dynamics to the deterioration of the general condition.
- The presence of advanced cardiac pathologies that developed against the background of a late visit to the doctor and the lack of adequate treatment.
- both congenital and acquired.
- Ischemic pathologies leading to the development of a heart attack.
Types of heart surgery
Today, there are many different surgical manipulations on the human heart. All these operations can be divided according to several basic principles.
- Urgency.
- Technique.
Operations differing in urgency
Any surgical intervention will fall into one of the following groups:
- emergency operations. The surgeon performs such heart operations if there is a real threat to the patient's life. It can be a sudden thrombosis, myocardial infarction, the onset of aortic dissection, heart injury. In all these situations, the patient is sent to the operating table immediately after the diagnosis is made, usually even without further tests and examinations.
- Urgent. In this situation, there is no such urgency, it is possible to conduct clarifying examinations, but it is also impossible to postpone the operation, as a critical situation may develop in the near future.
- Planned. After a long observation by the attending cardiologist, the patient receives a referral to the hospital. Here he undergoes all the necessary examinations and preparation procedures before surgery. The cardiac surgeon clearly sets the time of the operation. In case of problems, for example, a cold, it can be postponed to another day or even a month. There is no threat to life in such a situation.

Differences in technique
In this group, all operations can be divided into ongoing:
- Opening the chest. This is a classic method that is used in the most severe cases. The surgeon makes an incision from the neck to the navel and opens the chest completely. Thus, the doctor gets direct access to the heart. Such manipulation is carried out under general anesthesia and the patient is transferred to the cardiopulmonary bypass system. As a result of the fact that the surgeon works with a "dry" heart, he can eliminate even the most severe pathologies with a minimal risk of complications. This method is resorted to in the presence of problems with the coronary artery, aorta and other great vessels, with severe atrial fibrillation and other problems.
- Without opening the chest. This type of surgical intervention belongs to the so-called minimally invasive techniques. There is absolutely no need for open access to the heart. These techniques are much less traumatic for the patient, but they are not suitable in all cases.
- X-ray surgical technique. This method in medicine is relatively new, but it has already proven itself very well. The main advantage is that after these manipulations the patient recovers very quickly and complications are extremely rare. The essence of this technique lies in the fact that a device similar to a balloon is introduced to the patient using a catheter to expand the vessel and eliminate its defect. This whole procedure is carried out using a monitor and the progress of the probe can be clearly controlled.
The difference in the amount of assistance provided
All surgical manipulations in people with heart problems can be divided both in terms of the volume and direction of the problems to be eliminated.
- Correction is palliative. Such surgical intervention can be attributed to auxiliary techniques. All manipulations will be aimed at bringing blood flow back to normal. This may be the end goal or preparation of the vessel for further surgical procedures. These procedures are not aimed at eliminating the existing pathology, but only eliminate its consequences and prepare the patient for full treatment.
- radical intervention. With such manipulations, the surgeon sets himself the goal - if possible, the complete elimination of the developed pathology.

Most common heart surgeries
People with problems of the cardiovascular system are often interested in what types of heart surgeries are and how long they last. Let's look at some of them.
RF ablation
A fairly large number of people have problems with a violation in the direction of its increase - tachycardia. In difficult situations today, cardiac surgeons offer radiofrequency ablation, or "cautery of the heart." This is a minimally invasive procedure that does not require an open heart. It is performed using X-ray surgery. The pathological part of the heart is affected by radio frequency signals, which damage it, and therefore eliminate the additional path along which the impulses pass. Normal pathways are at the same time fully preserved, and the heart rate gradually returns to normal.
Coronary artery bypass grafting
With age or due to other circumstances, atherosclerotic plaques can form in the arteries, which narrow the lumen for blood flow. Thus, the flow of blood to the heart is greatly impaired, which inevitably leads to very deplorable results. In the event that the narrowing of the lumen reaches a critical state, surgery recommends that the patient undergo coronary artery bypass grafting.
This type of surgery involves creating a bypass from the aorta to the artery using a shunt. The shunt will allow blood to bypass the narrowed area and normalize blood flow to the heart. Sometimes it is required to install not one, but several shunts at once. The operation is quite traumatic, like any other, performed at the opening of the chest and lasts a long time, up to six hours. Coronary artery bypass surgery is usually performed on the open heart, but today alternative methods are gaining more and more popularity - coronary angioplasty (insertion of an expanding balloon through a vein) and stenting.
Like the previous method, it is used to increase the lumen of the arteries. It is referred to as a minimally invasive, endovascular technique.
The essence of the method consists in introducing an inflated balloon in a special metal frame into the artery into the pathology zone, using a special catheter. The balloon inflates and opens the stent - the vessel also expands to the desired size. Next, the surgeon removes the balloon, the metal structure remains, creating a strong skeleton of the artery. Throughout the procedure, the doctor monitors the progress of the stent on the screen of the X-ray monitor.

The operation is practically painless and does not require long and special rehabilitation.
Heart valve replacement
With congenital or acquired pathology of the heart valves, the patient is often shown their prosthetics. Regardless of what type of prosthesis will be installed, surgery most often takes place on the open heart. The patient is put to sleep under general anesthesia and transferred to the cardiopulmonary bypass system. Given this, the recovery process will be long and fraught with a number of complications.
An exception to the procedure for valvular replacement is aortic valve replacement. This procedure can be performed using a gentle endovascular technique. The surgeon inserts a biological prosthesis through the femoral vein and places it in the aorta.
Operations Ross and Glenn
Often, heart surgery is performed on children who are diagnosed with congenital heart defects. Most often, operations are performed according to the methods of Ross and Glenn.
The essence of the Ross system is to replace the aortic valve with the pulmonary valve of the patient. The biggest advantage of such a replacement can be considered that there will be no threat of rejection, like any other valve taken from a donor. In addition, the annulus will grow with the child's body and can last a lifetime. But, unfortunately, an implant must be placed in place of the removed pulmonary valve. It is important that the implant at the site of the pulmonary valve lasts much longer without replacement than the same one at the site of the aortic valve.
The Glenn technique was developed for the treatment of children with pathology of the circulatory system. This is a technology that allows you to create an anastomosis to connect the right pulmonary artery and the superior vena cava, which normalizes the movement of blood flow through the systemic and pulmonary circulation.
Despite the fact that surgical intervention significantly prolongs the life of the patient and improves its quality, it is still mostly an extreme case.
Any doctor will try to do everything possible so that the treatment is conservative, but, unfortunately, sometimes this is completely impossible. It is important to understand that any surgical intervention in the work of the heart is a very difficult procedure for the patient, and it will require high-quality rehabilitation, sometimes quite lengthy.
Recovery time
Rehabilitation after heart surgery is a very important stage in the treatment of patients.
The success of the operation can only be judged after the end, which can last quite a long time. This is especially true for patients who underwent open heart surgery. Here it is extremely important to follow the recommendations of doctors as accurately as possible and have a positive attitude.
After surgery with an opening of the chest, the patient is discharged home in about a week or two. The doctor makes clear instructions for further treatment at home - it is especially important to follow them.

trip home
Already at this stage, it is important to take measures so that you do not have to go back to the hospital urgently. It is important to remember here that all movements should be as slow and smooth as possible. In the event that the road takes more than one hour, you need to periodically stop and get out of the car. This must be done to avoid stagnation of blood in the vessels.
Relations with relatives
Both relatives and the patient need to understand that people who have undergone major operations under general anesthesia are extremely prone to irritability and mood swings. These problems will pass with time, you just need to treat each other with maximum understanding.
Taking medications
This is one of the most important moments in life after heart surgery. It is important for the patient to always have all the necessary medicines with him. It is especially important not to show excessive self-activity and not to take drugs that are not prescribed. In addition, you should not stop taking medication prescribed by your doctor.
seam care
The patient should calmly perceive a temporary sensation of discomfort in the suture area. In the beginning, it can be pain, a feeling of tightness and itching. Painkillers can be prescribed by a doctor to relieve pain; special ointments or gels can be used to relieve other symptoms, but only after consulting a surgeon.
The seam should be dry, without excessive redness or swelling. This needs to be watched closely. The place of the seam must be constantly treated with brilliant green, and the first water procedures are allowed to be taken after about two weeks. Such patients are allowed only a shower, and taking a bath and sudden changes in temperature are contraindicated. It is recommended to wash the seam only with ordinary soap and gently blot with a towel.
In a situation where the patient's temperature rises sharply to 38 degrees, severe swelling appears with redness at the site of the suture, fluid is released or severe pain is disturbing, you should immediately consult a doctor.
It is important for a person who has undergone heart surgery to set a goal - maximum recovery. But the main thing here is not to rush, but to do everything gradually and very carefully.
In the first days after returning home, you need to try to do everything as smoothly and slowly as possible, gradually increasing the load. For example, in the early days, you can try to walk from one hundred to five hundred meters, but if fatigue appears, you should rest. Then the distance should be gradually increased. It is best to walk outdoors and on flat terrain. After a week of walking, you should try to climb the stairs for 1-2 flights. At the same time, you can try to do simple housework.

Approximately two months later, the cardiologist will perform a stitch healing test and give permission to increase physical activity. The patient may begin to swim or play tennis. He will be allowed to work lightly in the garden with the lifting of small weights. Another test the cardiologist should conduct in three or four months. By this time, it is desirable for the patient to restore all the basic motor activity.
Diet
This aspect of rehabilitation also needs to be paid close attention.
The first time after the operation, the patient often lacks appetite and at this time any restrictions are not very relevant. But over time, a person recovers and his desire to eat familiar foods is restored. Unfortunately, there are a number of strict restrictions that will now always have to be observed. In the diet, you will have to severely limit fatty, spicy, salty and sweet. Cardiologists advise what you can eat after heart surgery - vegetables, fruits, various cereals, fish and lean meat. It is extremely important for such people to monitor their weight, and hence the caloric content of food.
Bad habits
Patients who have undergone heart surgery, of course, are strictly prohibited from smoking and using drugs. Drinking alcohol during the rehabilitation period is also prohibited.
Life after surgery can become full and rich. After a period of rehabilitation, many patients return to life without pain, shortness of breath and, most importantly, fear.