Causes of expansion of the heart shadow and mediastinum on a radiograph. X-ray signs of the causes of heart pain. Expansion and deconfiguration of the median shadow. The roots of the lungs are covered by the mediastinal shadow.
Fluorography (FLG) is a preventive method of examining the chest organs, carried out using X-rays. There are two types of fluorography - film and digital. Digital FLG has recently gradually replaced film FLG, as it is superior to it in a number of parameters: it allows reducing radiation exposure to the body, and also simplifies working with images.
The standard frequency of fluorographic examination is once a year. This frequency is relevant for adolescents and adults who do not have any special indications. At the same time, there are groups of people who are recommended to undergo fluorography 2 times a year. Among them:
- workers of tuberculosis dispensaries, sanatoriums, maternity hospitals;
- patients with chronic diseases (asthma, diabetes, ulcers, etc.);
- workers in areas where the possibility of tuberculosis infection and its spread is increased (kindergarten teachers).
Fluorography is a mass examination method for identifying hidden diseases of the thoracic cavity: respiratory tuberculosis, pneumoconiosis, nonspecific inflammatory diseases and tumors of the lungs and mediastinum, pleural lesions.
Based on fluorographic studies, individuals with suspected diseases of the chest organs are selected. Patients who have changes in the lungs or heart undergo x-rays.
The roots are compacted and expanded
 The root of the lung is formed by the main bronchus, pulmonary artery and vein, bronchial arteries, lymphatic vessels and nodes. This can occur due to swelling of large vessels and bronchi, or due to enlargement of the lymph nodes. This symptom is also described in the presence of focal changes in the lungs, decay cavities, along with other typical signs. In these cases, compaction of the roots of the lungs occurs mainly due to an increase in local groups of lymph nodes. This symptom is observed in smokers, when there is a significant thickening of the wall of the bronchi and compaction of the lymph nodes, which are constantly exposed to smoke particles.
The root of the lung is formed by the main bronchus, pulmonary artery and vein, bronchial arteries, lymphatic vessels and nodes. This can occur due to swelling of large vessels and bronchi, or due to enlargement of the lymph nodes. This symptom is also described in the presence of focal changes in the lungs, decay cavities, along with other typical signs. In these cases, compaction of the roots of the lungs occurs mainly due to an increase in local groups of lymph nodes. This symptom is observed in smokers, when there is a significant thickening of the wall of the bronchi and compaction of the lymph nodes, which are constantly exposed to smoke particles.
The roots are heavy
This radiological sign can be detected in the presence of both acute and chronic processes in the lungs. Most often, the heaviness of the roots of the lungs or the heaviness of the pulmonary pattern is observed with chronic bronchitis, especially with smoker’s bronchitis. This symptom, along with thickening and expansion of the roots, is also typical of chronic bronchitis of smokers. Also, this symptom, in combination with others, can be observed in occupational lung diseases, bronchiectasis, and cancer.
Strengthening the pulmonary (vascular) pattern
The pulmonary pattern is formed largely by the shadows of blood vessels: arteries and veins of the lungs. This is why some use the term vascular (rather than pulmonary) pattern. An increase in the pulmonary pattern is observed during acute inflammation of any origin, for example, ARVI, bronchitis, pneumonia. An increase in the pulmonary pattern is observed in congenital heart defects with enrichment of the small circle, heart failure, and mitral stenosis. But these diseases are unlikely to be an incidental finding in the absence of symptoms. Increased pulmonary pattern in inflammatory diseases, as a rule, disappears within a few weeks after the illness.
Fibrosis
Signs of fibrosis in the image indicate a history of lung disease. Often this can be a penetrating injury, surgery, or an acute infectious process (pneumonia, tuberculosis). Fibrous tissue is a type of connective tissue and serves as a substitute for free space in the body. In the lungs, fibrosis is largely a positive phenomenon.
Focal shadows (foci)
This is a type of pulmonary field darkening. Focal shadows are called shadows up to 1 cm in size. The location of such shadows in the middle and lower parts of the lungs most often indicates the presence of focal pneumonia. If such shadows are detected and the conclusion adds “increased pulmonary pattern”, “merging of shadows” and “uneven edges” - this is a sure sign of an active inflammatory process. If the lesions are dense and more even, the inflammation subsides. The location of focal shadows in the upper parts of the lungs is typical for tuberculosis.
Calcifications
Calcifications are round shadows, comparable in density to bone tissue. Most often, calcifications form at the site of the inflammatory process caused by Mycobacterium tuberculosis. Thus, the bacterium is “buried” under layers of calcium salts. In a similar way, a focus can be isolated in case of pneumonia, helminthic infestation, or when a foreign body enters. If there are a lot of calcifications, then it is likely that the person had fairly close contact with a patient with tuberculosis, but the disease did not develop. The presence of calcifications in the lungs should not cause concern.
Adhesions, pleuroapical layers
Adhesions are connective tissue structures that arise after inflammation. Adhesions occur for the same purpose as calcifications (to isolate the area of inflammation from healthy tissue). As a rule, the presence of adhesions does not require any intervention or treatment. Only in some cases, during the adhesive process, pain is observed. Pleuroapical layers are thickenings of the pleura of the apexes of the lungs, which indicates an inflammatory process (usually tuberculosis infection) in the pleura.
Sinuses are free or sealed
Pleural sinuses are cavities formed by folds of the pleura. As a rule, when describing the image, the condition of the sinuses is also indicated. Normally they are free. In some conditions, effusion (fluid accumulation in the sinuses) may occur. A sealed sinus is most often a consequence of previous pleurisy or trauma.
Changes from the diaphragm
Another common fluorographic finding is an anomaly of the diaphragm (relaxation of the dome, high standing of the dome, flattening of the diaphragm dome, etc.). Its causes: a hereditary feature of the structure of the diaphragm, obesity, deformation of the diaphragm by pleuro-diaphragmatic adhesions, previous inflammation of the pleura (pleurisy), liver diseases, diseases of the stomach and esophagus, including diaphragmatic hernia (if the left dome of the diaphragm is changed), diseases of the intestines and other organs abdominal cavity, lung diseases (including lung cancer).
The mediastinal shadow is widened/displaced
The mediastinum is the space between the lungs. The organs of the mediastinum include the heart, aorta, trachea, esophagus, thymus, lymph nodes and vessels. The expansion of the mediastinal shadow, as a rule, occurs due to an enlargement of the heart. This expansion is most often unilateral, which is determined by an increase in the left or right parts of the heart. The normal position of the heart can fluctuate significantly, depending on the person’s physique. Therefore, what appears to be a shift of the heart to the left on fluorography may be the norm for a short, overweight person. Conversely, a vertical or even “teardrop-shaped” heart is a possible normal option for a tall, thin person. In the presence of hypertension, in most cases, the description of the fluorogram will read “mediastinal widening to the left,” “heart widening to the left,” or simply “widening.” Less commonly, uniform expansion of the mediastinum is observed, this indicates the possibility of myocarditis and heart failure. A shift of the mediastinum on a fluorogram is observed with an increase in pressure on one side. Most often this is observed with an asymmetric accumulation of fluid or air in the pleural cavity, with large tumors in the lung tissue on the opposite side.
Norms
Normally, structural pathology is not visualized in the examined organs.
Diseases for which a doctor may prescribe fluorography
Bronchiectasis
Interpretation of the fluorographic report “stranded roots” may indicate the presence of bronchiectasis in the patient.
Pleurisy
The presence of the wording “sealed sinus”, as well as a note about changes in the diaphragm in the fluorographic report most often indicate a history of pleurisy.
Lung cancer
The interpretation of “strandy roots”, as well as a note of changes in the diaphragm in the fluorographic report may indicate that the patient has lung cancer.
Acute bronchitis
The interpretation of the fluorographic conclusion “increased pulmonary (vascular) pattern” is observed in acute inflammation of any origin, including bronchitis. Increased pulmonary pattern in inflammatory diseases, as a rule, disappears within a few weeks after the illness.
Pulmonary tuberculosis (miliary)
Acute respiratory viral infection
The interpretation of the fluorographic conclusion “increased pulmonary (vascular) pattern” is observed in acute inflammation of any origin, including ARVI. Increased pulmonary pattern in inflammatory diseases, as a rule, disappears within a few weeks after the illness.
Pulmonary tuberculosis (focal and infiltrative)
The location of focal shadows (foci) in the image (shadows up to 1 cm in size) in the upper parts of the lungs, the presence of calcifications (round-shaped shadows, comparable in density to bone tissue) is typical for tuberculosis. If there are a lot of calcifications, then it is likely that the person had fairly close contact with a patient with tuberculosis, but the disease did not develop. Signs of fibrosis and pleuroapical layers in the image may indicate previous tuberculosis.
Acute obstructive bronchitis
The interpretation of “increased pulmonary (vascular) pattern” in a fluorographic report can be observed in acute inflammation of any origin, including bronchitis. Increased pulmonary pattern in inflammatory diseases, as a rule, disappears within a few weeks after the illness.
Pneumonia
The interpretations “increased pulmonary (vascular) pattern”, “focal shadows (foci)”, “calcifications” may indicate the presence of pneumonia. The increased pulmonary pattern usually disappears within a few weeks after the illness. Signs of fibrosis in the image may indicate a history of pneumonia.
Mediastinal tumors and cysts are a large and heterogeneous group of neoplasms. Neoplasms in the mediastinum can form from tissues and organs that are normally located there, as well as from tissues that are displaced into the mediastinum due to disorders of embryonic development. This article briefly discusses only the formations that are of greatest importance in a doctor’s practice. For convenience of presentation, this article discusses pathological disorders in the mediastinal lymph nodes and some other disorders.
Clinical signs of mediastinal tumors and cysts can be different and depend on the size, nature (benign or malignant), and location of the tumor. Some mediastinal tumors do not show any clinical signs (for example, mediastinal cysts) and are detected during a preventive examination. In other cases, patients may complain of shortness of breath, cough, and chest pain. So, thymoma(tumor of the thymus) can be combined with myasthenia gravis. With malignant neoplasms, the patient complains of weakness and a sharp decrease in body weight. In the case of the development of large mediastinal neoplasms, superior vena cava compression syndrome(cyanosis of the upper half of the body, shortness of breath, dilation of the veins of the upper extremities and neck), and symptoms of compression of the esophagus and upper respiratory tract may also be observed. Recurrent nerve damage manifests itself dysphagia(impaired swallowing), damage to the phrenic nerves accompanied by relaxation of the diaphragm, and if the process involves sympathetic trunk, arises Horner's syndrome(ptosis, miosis, enophthalmos). In addition, symptoms of spinal cord damage may occur. Suppuration of mediastinal cysts causes inflammatory syndrome, increased body temperature.
Today, in the diagnosis of mediastinal formations, the leading role is played by X-ray computed tomography (XCT), and the task of traditional radiography is to detect changes in the X-ray picture that are suspicious for mediastinal pathology.
First of all, we need to consider some issues of the anatomy of the mediastinum. A detailed description of the anatomy of the mediastinum can be found in manuals on RCT; in traditional radiography, a somewhat simplified scheme is used.
On a lateral radiograph, the mediastinum is divided into 3 sections:
- Anterior mediastinum- from the posterior surface of the sternum to the anterior surface of the aorta and heart
- Central mediastinum- formed by the heart, aorta and aortic arch, trachea, the roots of the lungs also belong to the central mediastinum
- Posterior mediastinum- located behind the posterior surface of the heart and behind the trachea, also includes the descending aorta and esophagus
The mediastinum is also divided into top floor(located above the tracheal bifurcation) and ground floor(located below the tracheal bifurcation). Or the mediastinum is divided into three floors:
- Upper- above the level of the V thoracic vertebra
- Average- located at the level from the V thoracic vertebra (located approximately at the level of the tracheal bifurcation) to the VIII thoracic vertebra
- Lower- below the level of the VIII thoracic vertebra
The most common radiological sign of the presence of a neoplasm in the mediastinum is extension of the median shadow. At the same time, on the radiograph in a direct projection, smoothing of the arches formed normally by the aorta and the cardiac shadow is noted. The expansion of the mediastinum is also accompanied by the formation of “protrusions” (additional shadows of semicircular, semi-oval or irregular shape) along the contour of the mediastinum (on one or both sides), the wide base of which merges with the median shadow (Figure 1, 2). The contours of the extended median shadow are clear and even, and in the case of development malignant neoplasms- fuzzy and lumpy.

Figure 1. Neoplasm in the mediastinum (schematic image of a radiograph in frontal and lateral projections). In this image, the tumor belongs to the anterior mediastinum

Figure 2. Mediastinal mass. A - expansion of the mediastinal shadow to the left in the middle floor, caused by a neoplasm (see arrow). B- radiograph of another patient: the image shows an expansion of the mediastinal shadow with a polycyclic contour to the right in the upper floor, and an expansion (to a lesser extent) of the mediastinal shadow to the left (see arrows) is also noted.
The “belonging” of a pathological shadow to the mediastinum can be established in the following way: if on a radiograph in a direct projection one mentally extends the contours of the shadow to a full circle or oval, then the “center” of the shadow will be located outside the pulmonary field, in the mediastinum (Figure 3), and the “corners” “between the contour of the mediastinum and the shadow of the neoplasm there will be blunt. Also, shadows caused by neoplasms in the mediastinum do not correspond to the lobes and segments of the lung and can be projected onto several lobes at the same time (like other extrapulmonary formations, for example, encysted effusions; see article). It is necessary to pay attention to the fact that these signs do not “work” in all cases (for example, with neurogenic tumors that are localized in the posterior mediastinum near the shadow of the spine, the “center” of the shadow of the tumor is often projected not onto the mediastinum, but onto the pulmonary field).

Figure 3. Difference in projection of the tumor shadow (schematic image of a radiograph in direct projection). A- projection of the neoplasm into the mediastinum; B- intrapulmonary formation
On a lateral radiograph, an additional shadow may be detected in the corresponding part of the mediastinum, but it is not always clearly visualized, especially if the tumor is localized in the upper mediastinum. It is necessary to pay due attention to the analysis of the retrosternal space - in case of damage to the anterior mediastinum, it is obscured. If changes in the mediastinum are determined only on an X-ray in a direct projection, and pathological changes are not reliably detected on a X-ray in a lateral projection, the patient must undergo additional X-ray CT examination.
The most common mediastinal neoplasms
The expansion of the upper mediastinum is often caused by an enlargement of the thyroid gland - an intrathoracic goiter, which on a direct X-ray is defined as an expansion of the upper floor of the mediastinum due to an additional semi-oval or semi-circular shadow with usually clear and even contours, the base of which merges with the shadow of the mediastinum. Often this expansion of the mediastinal shadow occurs to the right, since the aortic arch deflects the goiter to the right (Figure 4), however, the mediastinal shadow can expand in both directions (Figure 5), especially if the goiter is large (Figure 6).

Figure 4. Intrathoracic goiter. A - X-ray in direct projection: the mediastinum in the upper floor is expanded to the right due to an additional formation with a clear and even contour (see arrow); the formation significantly displaces the trachea to the left (see pointers). B- radiograph in the right lateral projection: the goiter (see arrows) is located behind the trachea - in the posterior mediastinum

Figure 5. Intrathoracic goiter. The expansion of the mediastinum in the upper floor in both directions is determined, the contours of the shadow are clear and even (see arrows)

Figure 6. Large intrathoracic goiter. The goiter expands the mediastinal shadow in both directions; trachea is displaced to the right (see arrows)
When the goiter is located in the upper floor of the posterior mediastinum, the trachea usually shifts forward, which can be determined on a lateral radiograph. In some cases, the shadow of the goiter is not clearly visualized on the lateral projection image. In some cases, the shadow of the expanded upper mediastinum continues upward into the shadow of the soft tissues of the neck. Calcifications (clumpy, or in the form of diffuse calcification or a rim) may also be observed in the structure of the goiter. Note that intrathoracic goiter often causes compression of the superior vena cava, narrowing and displacement of the esophagus and trachea (Figure 7).

Figure 7. Displacement of the contrasted esophagus and trachea to the left by intrathoracic goiter. The shadow of the mediastinum is expanded due to the goiter to the right in the upper section (see arrow)
Lipomas
Lipomas are often localized in the anterior mediastinum, in the lower floor. Mediastinal lipoma on x-ray is usually defined as an irregularly rounded formation adjacent to the heart, anterior chest wall and diaphragm. In some cases, the shadow of a lipoma can merge with the cardiac shadow, thereby “simulating” an increase in the size of the heart.
Abdominomediastinal lipomas
So-called abdominomediastinal lipomas are found quite often. In fact, this is not a neoplasm, but a prolapse of fatty preperitoneal tissue into the mediastinum through slits in the diaphragm. The X-ray picture of abdomino-mediastinal lipomas is characterized by additional shadows of semi-circular, semi-oval or irregular shape in the lower floor of the anterior mediastinum, localized in the area of the cardiophrenic sinuses, often on the right. On a radiograph in a direct projection, abdominomediastinal lipomas are adjacent to the cardiac shadow and diaphragm; An x-ray in a lateral projection reveals obtuse “angles” formed by this lipoma with the diaphragm and the anterior wall of the chest (Figure 8, 9).

Figure 8. Abdominomediastinal lipoma (schematic illustration)

Figure 9. Abdominomediastinal lipoma in the right cardiophrenic sinus. A - radiograph in frontal projection, B - radiograph in right lateral projection
Coelomic pericardial cysts
Coelomic pericardial cysts have radiographic features similar to abdominomediastinal lipomas, but are less common and are localized in the cardiophrenic sinuses. On a radiograph, coelomic pericardial cysts are defined as a semicircular or semioval shadow. Experts note that on the X-ray in the lateral projection, the “angles” formed by the coelomic cyst with the diaphragm and the anterior chest wall are sharp (Figure 10, 11).

Figure 10. Coelomic pericardial cyst (schematic illustration)

Figure 11. Coelomic pericardial cyst. A - enlarged fragment of a radiograph in a direct projection: on the right, in the projection of the cardiophrenic sinus, a poorly visible additional semi-oval shadow with an even contour is determined (see arrow). B- radiograph in the right lateral projection: the shadow of the cyst above the diaphragm is clearly visible, located not strictly in the cardiophrenic sinus, but slightly posteriorly (see arrows)
Accurate differential diagnosis of abdominal-mediastinal lipomas and coelomic pericardial cysts can be made possible by performing RCT (RCT allows one to identify both an accumulation of adipose tissue and a cyst with fluid contents). Often additional shadows are found in the cardiophrenic sinuses due to moorings(massive fibrous layers on the pleura). Mooring lines are characterized by less convex contours, and their shape is similar to triangular (see article and)
Timoma
Thymoma is a tumor of the thymus gland. On a radiograph, thymoma is usually found in the anterior mediastinum, in the middle floor. Thymoma forms a pear-shaped or oval-shaped shadow with smooth, sometimes wavy contours. Experts believe that on a radiograph in a direct projection, benign thymomas usually expand the mediastinal shadow in only one direction, and on a radiograph in a lateral projection, the shadow may not be detected, since the thymoma has a flat configuration and has a low shadow intensity. Malignant thymomas are often identified on a lateral radiograph; the contours of the shadow of malignant thymoma are fuzzy and lumpy. The X-ray picture of malignant thymomas resembles lymphoma (see article).
Teratodermoid formations
Teratodermoid formations include teratoma And dermoid cysts- neoplasms of the mediastinum, formed as a result of disturbances in the development of tissues and organs during embryonic development, which contain tissues that are not characteristic of this anatomical region. On a radiograph, such formations are localized in the anterior mediastinum, in the middle floor (rarely in the upper floor) in the form of an additional shadow with a clear and even contour. In teratodermoid formations, calcifications, adipose tissue, a cystic component with liquid content, and bone inclusions (bone fragments, teeth) can be detected. When performing conventional radiography, such inclusions are rarely detected, that is, in most cases it is impossible to differentiate teratodermoid formations from other mediastinal neoplasms. Dermoid cysts sometimes break into the esophagus or bronchus (in this case, a horizontal liquid/gas level is detected in the formation on an x-ray). If teratodermoid formations are malignant, the contours of the shadow have fuzzy, bumpy contours; however, the exact nature of the formation can only be determined by performing a biopsy and further histological examination of the resulting biopsy.
Cysts
Cysts in the mediastinum may be bronchogenic(bronchial origin) and enterogenous(occur due to disruption of the digestive canal). Sometimes these types of cysts can only be differentiated by histological analysis. It is often very difficult to detect mediastinal cysts during routine radiography, since the shadows of these cysts may not extend beyond the contour of the midline. As a rule, mediastinal cysts are filled with contents (on an x-ray they are determined in the form of oval or rounded homogeneous shadows), and in the wall of bronchogenic cysts calcifications of the “shell” type can be detected.
Bronchogenic cysts often localized in the central mediastinum, in the upper or middle floor, near or under the tracheal bifurcation, and also close to the main bronchi. In this case, the radiograph shows in a limited area an expansion of the median shadow with a clear arc-shaped contour.
Enterogenous cysts often located in the posterior mediastinum (more precisely, in that part of the posterior mediastinum that is located anterior to the spine - in Holtzknecht's space), in the lower floor, close to the esophagus.
Mediastinal cysts can compress and displace the trachea and esophagus. In the event of a cyst breakthrough into the esophagus, bronchus or trachea, a thin-walled cavity with a horizontal level of liquid/gas contents is detected on the x-ray.
Neurogenic tumors
Neurogenic tumors form in the mediastinum from the sheaths of peripheral nerves ( neurofibroma, schwannoma), as well as from the sympathetic and parasympathetic ganglia ( neuroblastomas, ganglioneuromas). Such neoplasms are localized in the paravertebral space - the costovertebral groove - traditionally belong to the posterior mediastinum and can be found in any floor (upper, middle, lower).
On an x-ray, neurogenic tumors are identified as additional shadows of an oval (semi-oval) or round (semi-circular) shape with clear, even contours. In the later stages of tumor development, the contours of the shadow may become unclear and uneven (lumpy). In some neurogenic tumors, calcifications may be detected. In addition to the expansion of the median shadow, an additional shadow is detected on radiographs in frontal and lateral projections, which is visualized against the background of the spine or adjacent to the spine. It is sometimes difficult to differentiate neurogenic tumors from intrapulmonary neoplasms, since when a neurogenic tumor grows towards the lung, it projects predominantly onto the pulmonary field. Neurogenic tumors can also cause changes in adjacent bone structures - deformation and usuration of the ribs and vertebrae due to pressure, expansion of the intervertebral foramina.
If a mass formation of the mediastinum is suspected, the patient must be prescribed an RCT to clarify the location and structure of the formation (presence of fluid, inert tissue, calcifications, adipose tissue, cystic component in the formation), determine the signs of a malignant process, and detect enlarged lymph nodes in the mediastinum.
Other causes of widening of the mediastinal shadow
Esophageal diverticula
Diverticula of the esophagus occur in any part of the esophagus and can cause widening of the median shadow. "Cervical" (Zenker's) diverticula esophagus are localized in the upper part of the mediastinum. Diagnosis of diverticula by radiography requires contrast examination of the esophagus.
Aortic aneurysm
Aortic aneurysm may cause expansion of the median shadow. With an aneurysm of the ascending aorta, the median shadow expands to the right; with an aneurysm of the descending aorta, the median shadow expands to the left (Figure 12, 13)

Figure 12. Aneurysm of the descending aorta (see arrow). A- radiograph in direct projection; B- radiograph in the left lateral projection.

Figure 13. Aneurysm of the descending aorta. A - X-ray in direct projection: there is a significant expansion of the median shadow to the left due to the aorta. B- radiograph in the left lateral projection: the expansion of the entire descending aorta is determined
Note that an aneurysm of the descending aorta in its lower section (above the diaphragm) on an x-ray can simulate changes in the lung (additional round formation) or a hiatal hernia (see Figure 14).

Figure 14. Aneurysm of the descending aorta located supradiaphragmatically. A - X-ray in direct projection: in the lower part of the mediastinum is expanded to the left due to an additional shadow, which is partially defined behind the heart (see arrow). B- radiograph in the left lateral projection: an additional shadow is identified above the diaphragm, which is a “continuation” of the shadow of the descending aorta (see arrows)
Please note that on an x-ray, aortic dissection is not always identified as dilation of the aorta, since in some cases dissection occurs in the absence of an aortic aneurysm. An existing aortic aneurysm can also be complicated by dissection. If aortic dissection is suspected, the patient should undergo multispiral CT with angiography.
Abnormalities in the location of the aorta, such as a right-lying aorta, can cause the median shadow to expand to the right. In this case, the aortic arch and descending aorta in a typical place (along the left contour of the median shadow) are not determined, since they are located on the right (Figure 15)

Figure 15. Right aorta. A - X-ray in direct projection: in the upper part, the expansion of the mediastinal shadow to the right is determined, in a typical location on the left, the aortic arch is not visualized. B- radiograph in the right lateral projection: the aortic arch is identified behind the trachea (see arrow)
Hiatal hernia
Large hiatal hernias can cause widening of the median shadow in the lower part. On a lateral X-ray, such hernias are revealed behind the shadow of the heart in the form of additional round-shaped formations (rarely irregularly rounded) with clear contours. As a rule, they determine the horizontal level of the contents that is in the stomach; less often, this level is not determined. Diagnosis of hiatal hernia is carried out by contrast examination of the esophagus and stomach (Figure 16).

Figure 16. Intrathoracic location of the stomach. A - X-ray in direct projection: in the lower part of the mediastinum, an expansion of the mediastinal shadow to the right is determined (see arrow). B- radiograph in the right lateral projection: an additional shadow behind the heart is determined (see arrows); This is a somewhat atypical picture, since the liquid/gas level typical for the stomach is not visualized. IN- contrast study of the stomach: the stomach is almost completely located towards the chest cavity (this is due to the “short esophagus”)

Figure 17. Expansion of the mediastinum due to a giant aneurysm of the aberrant subclavian artery on the right

Figure 18. A - X-ray taken in the supine position: the expansion of the mediastinal shadow in the upper part to the right is determined. B- X-ray of the same patient in a standing position: the mediastinal shadow is not widened
22.02.2017
When examined in direct projection, the mediastinal organs form an intense, so-called median shadow, represented mainly by the heart and large vessels, which projectionally overlap the remaining organs.
Direct projection. When examined in direct projection, the mediastinal organs form an intense, so-called median shadow, represented mainly by the heart and large vessels, which projectionally overlap the remaining organs.
The shadow of the mediastinum is delimited laterally by the lungs, from below it merges with the medial sections of the domes of the diaphragm, at the top it noticeably narrows and smoothly passes directly into the neck area. The outer contours of the mediastinal shadow are clearly demarcated from the lungs, they are more convex at the level of the edge-forming contour of the heart and the areas of the vascular bundle are somewhat straightened, especially on the right with the edge-forming location of the superior vena cava. Extending outward and upward from the upper pole of the vascular bundle, the brachiocephalic trunk on the right and the subclavian artery and vein on the left form clearly defined shadows with somewhat bent contours, which lose their differentiated image at the level of the sternal ends of the clavicles.
The upper part of the mediastinum looks less intense and homogeneous, since the trachea is projected in the middle, forming a longitudinally located light strip about 1.5-2 cm wide.
The mediastinal lymph nodes normally do not provide a differentiated image. They are visible only when they are enlarged (Fig. 230), calcified or with contrast (lymphography).
The shape and size of the median shadow largely depend on the age and constitutional characteristics, breathing phase and position of the patient. In people with an asthenic build, the mediastinum is narrower and longer, in hypersthenics it is wider and shorter than in normosthenics. The mediastinum changes shape and size with different phases of breathing and changes in body position: during inspiration there is a moderate decrease in the transverse size of the mediastinum, and during exhalation there is a slight expansion of it.
When breathing, the median shadow, changing its transverse size, does not make noticeable lateral displacements. Lateral jerky displacements of the median shadow during fast and deep inspiration are one of the signs of impaired bronchial obstruction.
When examined in a horizontal position, the transverse size of the mediastinum is larger than in a vertical position. When the torso is tilted and examined on the side, a lateral displacement of the mediastinum of up to 2-3 cm is observed.
This should be kept in mind when determining the depth of the tomographic slice in the lateral projection. Sufficient displacement of the mediastinum indicates the absence of adhesions and tumor invasion of the mediastinum.
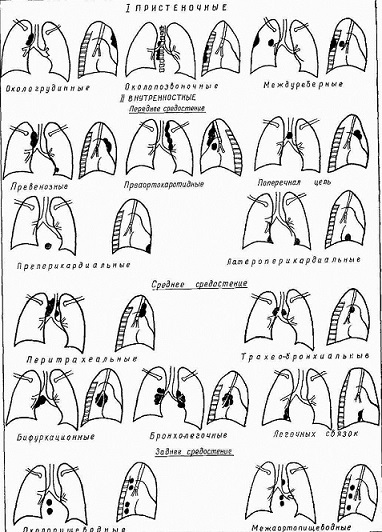
Rice. 230. Schematic representation of the topography of enlarged intrathoracic lymph nodes.
Lateral projection. When examined in a lateral projection, the organs of the mediastinum, due to less projection layering and natural contrast, are visible more clearly than in a direct projection. In this projection, the boundaries of the mediastinum are clearly visible: in front - the sternum, behind - the thoracic postures, below - the diaphragm, above - the upper opening of the chest.
Radiologically, when examining in a lateral projection, it is possible to draw the boundaries according to the conditional division of the mediastinum into anterior, middle, posterior, superior and inferior.
The division of the mediastinum into these sections is carried out by drawing two frontal planes, respectively, of the anterior and posterior walls of the trachea and one horizontal plane - downward from the bifurcation of the trachea.
This division of the mediastinum is of practical importance in the differential diagnosis of various pathological processes, since clarifying the localization of the detected formations narrows the range of diseases that must be taken into account in each specific case.
The anterior mediastinum in the x-ray image is projected between the posterior surface of the sternum and the vertical line drawn along the anterior wall of the trachea. In its upper part in adults, the shadow of the ascending aorta is visible, the anterior contour of which bulges somewhat anteriorly, is clearly defined, directed upward and posteriorly and passes into the shadow of the aortic arch. In children, the thymus gland is located anterior to the ascending aorta. The anterior marginal sections of both lungs are projected onto the anterior mediastinum anterior to the ascending aorta, and therefore its transparency increases. The triangular-shaped area of clearing, delimited in front by the sternum, below by the heart, and behind by the ascending aorta, is called the retrosternal space. Against its background, the vessels of the anterior segments of the upper lobes can be traced. The high transparency of the retrosternal spaces should be taken into account when recognizing pathological processes of the anterior mediastinum, since even massive pathological formations (enlarged prevascular lymph nodes, tumors and mediastinal cysts) can produce shadows of low intensity as a result of the “weakening” effect of the projected air lung tissue.
The lower part of the anterior mediastinum is occupied by the shadow of the heart, against which the vessels of the middle lobe and lingular segments are projected.
The middle mediastinum in the upper section has a heterogeneous structure, as a result of a clear image in the air column of the trachea, down from which the shadows of the roots of the lungs are projected onto the mediastinum. The lower part of the middle mediastinum is also occupied by the heart. In the posterior cardiophrenic angle there is a shadow of the inferior vena cava.
The posterior mediastinum is projected between the posterior wall of the trachea and the anterior surface of the thoracic vertebral bodies. In the X-ray image, it has the appearance of a longitudinally located strip of clearing, against which in elderly people a vertically located shadow of the descending aorta about 2.5-3 cm wide is visible. The intensity of the aortic shadow gradually decreases downwards.
The upper part of the posterior mediastinum is blocked by the muscles of the upper shoulder girdle and shoulder blades, due to which it has reduced transparency.
As a result of the projection summation of the shadow of the scapula and the aorta (at the level of the transition of the descending aortic arch), an intense homogeneous shadow with a clear anterior contour, corresponding to the posterior wall of the trachea, and a less clear and convex upper contour of the aortic arch is often determined. Sometimes this shadow, caused by these anatomical formations, is mistaken for enlarged lymph nodes or a tumor of the posterior mediastinum.
Rice. 231. Schematic division of the mediastinum on a radiograph in the lateral projection (according to Thwing).
The lower part of the posterior mediastinum, delimited by the heart, diaphragm and vertebrae, has greater transparency and is called the retrocardial space. Against the background of the latter, the vessels of the main segments of the lungs are projected.
Normally, the transparency of the retrosternal and retrocardial spaces in its lower part is almost the same. Complete or partial darkening of the retrosternal and retrocardial spaces, as well as the appearance of additional shadows at the level of the mediastinal organs (heart, aorta, trachea) indicate the presence of a pathological process. Thus, the lateral projection is optimal for x-ray examination of the mediastinum.
Thwining (1939) proposed an even more detailed division of the mediastinum into 9 parts. This schematic division is achieved by drawing two vertical lines in the frontal and two horizontal planes (Fig. 231).
The boundary between the anterior and middle mediastinum is drawn along a vertical line connecting the sternoclavicular joint and the anterior part of the diaphragm at the place of its projection intersection with the pleura oblique fissure. The posterior mediastinum is separated from the middle by the frontal plane, which runs slightly posterior to the trachea. The dividing line between the upper and middle mediastinum runs horizontally at the level of the body of the V thoracic vertebra, and between the middle and lower - horizontally, drawn at the level of the body of the VIII or IX thoracic vertebra.
X-ray anatomy of the mediastinal organs: heart and large vessels, trachea and main bronchi, esophagus and thymus is presented in the relevant sections of the manual.
Tags: mediastinum, median shadow, lymph nodes, styling, lateral projection
Start of activity (date): 02/22/2017 12:36:00
Created by (ID): 645
Key words: mediastinum, median shadow, lymph nodes, styling
| Tags: , |
The mediastinum is a part of the thoracic cavity, limited in front by the sternum, partially by the costal cartilages and retrosternal fascia, behind by the anterior surface of the thoracic spine, the necks of the ribs and the prevertebral fascia, on the sides by the layers of the mediastinal pleura, below by the diaphragm, and above by the horizontal plane, passed through the upper edge of the manubrium of the sternum.
To this day, the scheme for dividing the mediastinum, proposed by Twining in 1938, has not lost its significance. The two horizontal planes drawn (above and below the roots of the lungs) and two vertical planes (in front and behind the roots of the lungs) make it possible to distinguish three sections in the mediastinum: anterior, central, posterior and three floors: upper, middle, lower.
The division of the mediastinum into the listed sections makes it possible, based on x-ray examination, to clearly determine the localization of the pathological formation.
Diseases of the mediastinum have various radiological manifestations, in the form of diffuse or limited expansion of the median shadow; changes in the structure of the median shadow and displacement of the mediastinal shadow.
Limited expansion of the median shadow may be due to: tumors, cysts of the anterior and posterior mediastinum; conglomerate of lymph nodes; aortic aneurysm and the right aorta.
Among tumors of the anterior mediastinum that cause limited expansion of the median shadow, thymomas are found most often. They can occur at any age, mainly in patients in the fifth and sixth decades of life.
Rice. 1a,b. B-noy K. born in 1938. Survey radiographs of the chest organs in frontal and left lateral projections.
The mediastinum at the level of the anterior segments of the fourth ribs is expanded to the left by an additional formation located in the middle and lower floors of the anterior part of the mediastinum. Its outer contours are clear, the surface is smooth.
Rice. 2a,b,c,d. CT angiography. In the middle and lower floors of the anterior mediastinum, there is an irregularly shaped, cystic-solid structure, with clear contours, a formation, the upper pole of which is located under the aortic arch, and the lower pole reaches the diaphragm. Due to the introduction of a contrast agent, its density unevenly increases. The bifurcation of the trachea, the left main bronchus, and the pulmonary artery are moderately pushed to the right.
Conclusion: thymoma, given its clear contours, is most likely of a benign nature.
Histological examination of postoperative material - thymoma, type AB.
It should be remembered that when an additional formation is detected in the anterior mediastinum, differential diagnosis must be carried out with a retrosternal goiter; malignant tumors of the thymus gland, thymus cysts; dermoid cysts and teratomas; aneurysm of the ascending aorta, enlarged lymph nodes and sternocostal hernias of the diaphragm.
When there are any signs of disease, and a visual examination of the patient cannot provide clear information about the condition of a particular internal organ, doctors prescribe x-ray examinations. X-ray of the mediastinal organs is one of the leading methods for diagnosing existing pathological processes. Let's find out what kind of procedure this is and what diseases will be reflected in the finished image.
Indications and prohibitions for the procedure
Radiography of the mediastinum is performed at the initial stage of examining the patient. The procedure is painless and more accessible compared to computed tomography.
Reasons why radiation diagnostics may be prescribed:
- complaints of chest pain;
- coughing,
- labored breathing;
- enlarged cervical lymph nodes (their clear visualization);
- injuries to the esophagus, ribs and upper spine.

As in cases of examination of other organs, X-rays of the mediastinum are not performed on pregnant women (especially in the 1st trimester). If the question of diagnostics is urgent, and there are compelling reasons for this, then during exposure precautions should be taken, including protecting the patient's abdomen and pelvic area with a lead apron. There are no other contraindications to the procedure. Despite this, it is important not to forget that minimal radiation exposure is still present, so it is better not to undergo plain radiography of the organ too often.
There is no special preparation for undergoing mediastinal radiography. There are also no requirements regarding food and drink. The only thing you need to do is take off all your jewelry and remove metal objects from your pockets. During the image, the patient stands, pressing his chest against the shield and holding his breath. The picture is taken in lateral and frontal projection.
What will the photo show?
Before you start deciphering the image, it is worth finding out what kind of organ it is - the mediastinum. Essentially, this is a space that is localized in the chest and has clear boundaries.
For ease of diagnosis, the mediastinum is divided into three sections, each of which includes certain organs:
- Anterior section: vessels, lymphoid nodes, thymus gland;
- Middle section: bronchi, pulmonary veins and arteries, lymph nodes, heart, trachea, pericardium;
- Posterior section: esophagus, thoracic ducts, descending aorta.

Thanks to this division, it is possible to make an assumption about the nature, structure and cause of the formation of the mediastinum, which was shown by x-ray. When it comes to diagnosing benign tumors, their localization is of paramount importance. For example, intrathoracic and retrosternal goiter, which gives an expansion of the shadow of the mediastinum on x-ray, is formed in the upper part of the mediastinum, and brochoenterogenic cysts are near the esophagus.
An image made using the right technology will show:
- two or three vertebrae;
- location of the spinous processes between the clavicles (in the center);
- muscles of the diaphragm located at the level of the 6th rib;
- the shadow and any formations are clearly visualized.
Before proceeding with a detailed analysis, a radiologist conducts an initial study and writes a conclusion on it. It contains a brief description of the location and condition of the organs, information about the presence of enlargement, shadows or tumors.

Decryption algorithm
After writing a brief report, the radiologist begins a detailed analysis of the image. What diseases can he see?
- Pneumonia. Additional tissues are clearly visible in lateral and frontal projection images.
- Tuberculosis. This disease is characterized by increased venous pattern in the upper parts of the lung.
- Congestive failure. Manifested by an enlarged heart.
- Pleurisy. The image shows that the trachea is being pulled forward, which is due to the accumulation of fluid in this area.
- Pulmonary edema. Flaky darkening in the mediastinum indicates the presence of this pathology.
- Goiter. Expansion of the mediastinum on x-ray in one or both directions is the main sign of goiter. Also, along with the expansion of the shadow, a narrowing of this area can also be observed. Shadows can be cleared, compacted and with foci of calcification.

The detected mediastinal tumor on x-ray deserves special attention. Any neoplasm requires a more detailed diagnosis, which will include:
- clarification of location relative to other organs;
- determination of the shape, contours, structure of the tumor;
- assessment of behavior and characterization of the neoplasm.
It is important to remember that reading a finished X-ray is a very difficult task, since the image is a collection of heterogeneous structures layered on top of each other. Therefore, only a highly qualified specialist with extensive experience can perform the analysis accurately and correctly. This determines whether he will see the disease at an early stage of development.