OtoRead audiometer - OAE (otoacoustic emission) recording system. Hearing testing by recording delayed evoked otoacoustic emissions
5. STUDY OF HEARING BY REGISTRATION OF DELAYED OTOACUSTIC EMISSION
Otoacoustic emission is an acoustic response that is a reflection of the normal functioning of the auditory receptor. It's extremely weak sound vibrations, generated by the cochlea, which can be recorded in the external auditory canal using a highly sensitive microphone. These oscillations are the result of active mechanical processes occurring in the organ of Corti, namely in the outer hair cells. Active movements the latter, amplified due to positive feedback, are transmitted to the basilar membrane, inducing reversely directed traveling waves that reach the foot plate of the stapes and lead to the corresponding oscillatory process of the chain auditory ossicles, eardrum and air column in the external auditory canal.
There are spontaneous and evoked otoacoustic emissions. Spontaneous otoacoustic emissions can be recorded in the human external auditory canal in the absence of sound stimulation. Evoked otoacoustic emissions are recorded in response to sound stimulation and, in turn, are divided into several subtypes. However, during audiological examination of children in the first year of life, as a rule, only delayed evoked otoacoustic emissions (DEOAEs) are used, which occur within a certain period of time after the presentation of an acoustic stimulus. In reality, when recording TEOAE, sound pressure fluctuations are measured. It is for these purposes that the outer one is obturated during measurements. ear canal, which helps convert eardrum displacements into sound pressure. In addition, the effects of external noise are thus eliminated.
In individuals with normal hearing, the thresholds for the occurrence of TEOAE are very close to the subjective hearing thresholds. Distinctive feature TEOAE is that in the presence of sensorineural or conductive hearing loss, accompanied by an increase in hearing thresholds to 30 dB or more, the emission ceases to be registered.
Rice. 1. Otoacoustic emissions recorded in a newborn with normal hearing.
TEOAE consists of 2-3 (rarely more) groups of oscillations of different frequencies, occurring 6-8 ms after the onset of the stimulus and lasting for 20-30 ms. As already noted, their amplitude is very small. To record TEOAE, a probe is inserted into the external auditory canal, the housing of which contains a miniature telephone and microphone. The stimuli are broadband acoustic clicks presented at a repetition rate of 20-50/s. More frequent repetition of stimuli is also acceptable. The response signal picked up by the microphone is amplified with a bandwidth of 500 to 5000 Hz and sent to the computer through an analog-to-digital converter. Typically, to obtain a clearly identifiable response, it is necessary to average 250-500 post-stimulus segments of 20-30 ms each.
TEOAE can be registered in children as early as 3-4 days after birth (see Fig. 1). Considering the mentioned high sensitivity TEOAE even to minor impairment functional state organ of hearing, we can come to the conclusion that there is an excellent opportunity to use its registration as a method for conducting mass hearing examinations in children in the first years of life.
6. FACTORS AFFECTING THE RESULTS OF REGISTRATION OF TEOAE
In the absence of high-amplitude TEOAE, it is necessary to differentiate whether this is a consequence of pathology of the inner or middle ear, or the result of inadequate recording conditions. To date, there are eight factors that can influence the results of TEOAE registration or their interpretation: (1) the number of accumulated responses, (2) the adequacy of the stimulus, (3) the repeatability of the results, (4) the stability of the probe, (5) the condition of the child, (6) the presence of postpartum masses in the external auditory canal, (7) the timing of testing; (8) software for TEOAE analysis.
1. Number of savings. When a relatively small number of realizations accumulate, TEOAE may be present, but it is masked by noise. An increase in the number of accumulations is accompanied by an increase in the intensity of TEOAE and its prevalence over noise.
2. Adequacy of stimulation. Low stimulation intensity (less than 71 dB PE SPL) may be accompanied by an inadequately weak response, which does not depend on the functional state of the cochlea.
3. Repeatability. A decrease in noise intensity is accompanied by an increase in the percentage of repeatability of results. However, the change in response characteristics is not solely a function of stimulus intensity, which typically remains relatively constant throughout testing.
4. Probe stability. When the intensity of TEOAE changes during the recording process, correction of the probe installation leads to increased stability and an increase in the amplitude of TEOAE.
5. The child's condition. The duration of testing depends on the child's condition. Time required to test both ears in different stages sleep is 3.3-3.6 minutes, while testing both ears in an awake or crying child can last up to 20 minutes.
6. Effects of obstruction of the external auditory canal and the condition of the middle ear. Bad influence the results of TEOAE registration are influenced by postpartum masses and fluid in the external auditory canal, as well as negative pressure in tympanic cavity.
Therefore, before recording TEOAE, it is recommended to perform an otoscopy and clean (if necessary) of the external auditory canal. If the test results are negative, the child should undergo tympanometry (see below) to exclude middle ear pathology.
7. The optimal time for the first registration of TEOAE is the 3-4th day after the birth of the child, when the external auditory canal is already free of foreign matter and emission registration is most effective.
8. Software, used in the analysis of TEOAE. As a rule, two programs are used: quick screening and basic program. Rapid screening was developed to reduce the effects of low-frequency noise on TEOAE. If in the basic program the analysis window is 20 ms, then in the fast screening it is 12.5 ms, which is accompanied by a significant increase in the speed of click presentation.
If the child does not pass the test, he is scheduled for a repeat test, usually after 4-6 weeks. If the results of re-registration of TEOAE are negative, a study based on recording short-latency auditory evoked potentials (SLEP) is prescribed to confirm hearing impairment and determine the degree of its reduction.
It should be remembered that registration of TEOAE does not replace registration of KSVP, but only complements it. This is due for the following reasons:
1. The results obtained when recording TEOAE mainly reflect information about the activation of mid-frequency areas of the cochlea, while when registering CVEP, mainly high-frequency information is provided;
2. TEOAE is generated by outer hair cells and reflects micromechanical processes in the organ of Corti, while CVOAEs are the result of electrical activity of the auditory nerve and the nuclei of various structures of the auditory pathway.
3. TEOAE does not allow one to judge the degree of hearing loss, whereas when recording CVEP, it is possible to fairly reliably estimate hearing thresholds in the mid- and high-frequency regions.
7. AUDIOLOGICAL STUDY BASED ON REGISTRATION OF SHORT-LATENTE AUDIOUS EVOKED POTENTIALS
Objective audiometry, based on recording various classes of auditory evoked potentials, is quite widely used in Lately to determine the functional state of the hearing organ in children early age. The method is based on the fact that the conduction and processing of nerve signals in the auditory system are accompanied by specific electrical activity that differs from background activity brain. The amplitude of the resulting potentials is so small that it is not possible to identify them using conventional electroencephalography (EEG).
The problem is solved using the technique of averaging EEG segments immediately following the presented acoustic stimuli. When averaging, the amplitude of the useful signal, i.e., evoked potentials, increases in proportion to the number of accumulated EEG segments (N), while the amplitude of background activity and artifacts of muscular and other origin (the so-called “noise”) increases in proportion. Thus, than larger number accumulations, the higher the signal-to-noise amplitude ratio and, therefore, the easier the identification of evoked potentials. However, too big number accumulation leads to an unjustified lengthening of the examination time, therefore, in each specific case, a reasonable compromise is necessary between the number of averagings and the clarity of the resulting evoked potential curve.
To record evoked potentials of any generation levels, electrodes are needed that are installed at certain points on the head, an amplifier of bioelectrical activity, an analog-to-digital converter capable of transforming the signal into a form suitable for computer processing, and, finally, the computer itself, which carries out accumulation, averaging, storage and subsequent processing of evoked potentials.
In audiological studies, short-latency auditory evoked potentials (SLEPs) are most widely used. They occur 1.5-2 ms after the onset of the sound stimulus and last up to 10 ms. CVEPs consist of a complex of waves, the positive peaks of which are indicated in the order of their occurrence by Roman numerals (waves I-VII). Today, we can say with confidence that wave I (and possibly wave II) of SEP is generated by the auditory nerve. The remaining CVEP waves can be considered as the result of the total activity of many generators located in the structures of various levels of the auditory pathway.
Short acoustic clicks with a duration of 0.1 ms of variable polarity are most often used as stimuli when recording SEPs. The use of additional low-frequency tone bursts with a frequency of 250 Hz (1 cycle – rise time, 1 cycle – fall time) helps to expand information about the state of the child’s hearing.
With the standard method of recording CVEP, the frequency of stimulus presentation is 11-21/s. To exclude possible interaction of the stimulus with the electrical effects of the mains frequency (50 Hz), it is recommended (if possible) to use fractional number presentations – 11.1 Hz; 21.1 Hz, etc.
In order to exclude the possibility of collapse of the external auditory canal in newborns, as well as to reduce stimulus artifact, the use of in-ear phones is recommended.
One of the recording electrodes (positive) is usually placed on the vertex or along midline forehead at the border of hair growth; the second (negative) is placed on the mastoid process or earlobe ipsilateral to the sound stimulation; The grounding electrode is usually fixed on the mastoid process contralateral to the stimulus or the lobe of the contralateral ear. It should be borne in mind that in some cases the amplitude of the CVEP can be increased due to the location of the negative electrode in the area of the projection of the 7th cervical vertebra.
When using a conventional protocol, the driven activity is amplified with an amplifier bandwidth of 100-300 Hz ( bottom line bandwidth) up to 1500-3000 Hz ( upper limit bandwidth). However, given that CVEP in newborns is characterized by a significant presence of a low-frequency spectrum, it is recommended to use a band from 30 to 3000 Hz, which is also accompanied by optimization of the signal-to-noise ratio. The duration of the averaged EEG segments (analysis window) is usually 15-20 ms from the beginning of the stimulus. To obtain a clear SEP, it is enough to perform about 2000 averagings of post-stimulus EEG segments. It should be noted, however, that at near-threshold intensities of sound stimulation and/or when the child is restless, the indicated number of averagings is not enough. In such cases, it is recommended to increase the number of savings (for example, up to 4000).
Bibliography
1. V. F. Undrits, K. L. Khilov, N. N. Lozanov, V. K. Suprunov. Diseases of the ear, nose and throat (a guide for doctors). Publishing house "Medicine", 1969.
2. Medical scientific and practical journal "Bulletin of Otorhinolaryngology" No. 6, 1996
3. N.A. Nadeina. Clinical and audiological expert review hearing impairment. Research Institute of Medical and Social Expertise and Rehabilitation.
4. Diagnosis and correction of impaired auditory function in children of the first year of life. Almanac of the Institute of Correctional Pedagogy 3/2001\ Archive of the IKP Almanac.
5. F.A. Samsonov, A.I. Kryukov. Algorithm for examination and treatment of patients with sensorineural hearing loss. CONSILIUM-MEDICUM, Volume 2/N 8/2000
Idea of size eyeballs(buphthalmos, microphthalmos), cornea sizes (micro and macrocornea). The depth of the anterior chamber, the size and reaction to light of the pupil, the condition of the pupillary area (mydriasis, coloboma), etc. Methods for studying the eyelids, connective membrane, cornea, iris. The examination of the patient begins with an examination of the eyelids, during which the condition of the skin and the edges of the eyelids is established, ...




Twice as bad as normal child. Speech underdevelopment is manifested in a significant deviation from the norm in the formation of phonetic concepts underlying sound analysis. For younger children school age Speech underdevelopment is characterized by impaired reading expressiveness, lack of necessary pauses defined by punctuation marks, non-observance of pauses at the end of sentences, abrupt...
The second version of the operation is used, and if it does not improve hearing, the third one is used. Indirect method The operation is performed under local anesthesia through a regular ear specula inserted into the ear canal using a binocular magnification with a 2-2% magnification and a surgical microscope with 10-, 16-fold magnification. It is necessary to use suction; as a tip to it...
Audiology studies the specifics of work auditory organ. The clinical direction within which it occurs is called audiology.
The main research method is. Special electronic-acoustic devices are used for studying. With their help, the subjective reaction “I hear or I don’t hear” is assessed.
Another method is to study hearing through live speech. Speech is used for tests:
- conversational,
- in a whisper,
- loud,
- very loud.
When testing using whispered speech, it is recommended to pronounce words in a whisper after physiological exhalation using reserve air in the lungs.
When using normal speech, words are pronounced with average volume.
The evaluation criterion is the distance from the subject to the doctor. A person must confidently voice 8 out of 10 words.
Loud speech is made directly near the ear. This research method is used for third degree hearing loss.
Simple hearing diagnostics:
Indications
Rumor in mandatory tested in newborn children using instrumental research methods, and in workers who work in noisy industrial conditions. The functioning of the hearing organ is also checked during the driver's examination.
In all these cases, diagnosis is mandatory even in the absence of any complaints. If there are problems, tests are carried out before and after treatment is prescribed.
Indications may be:
- adenoids,
- ear diseases,
- necessity ,
- pathologies of the central nervous system,
- appearance of signs,
- heads.
Hearing tests
There are several techniques that allow you to assess the level of functioning of the hearing organ. Among them:
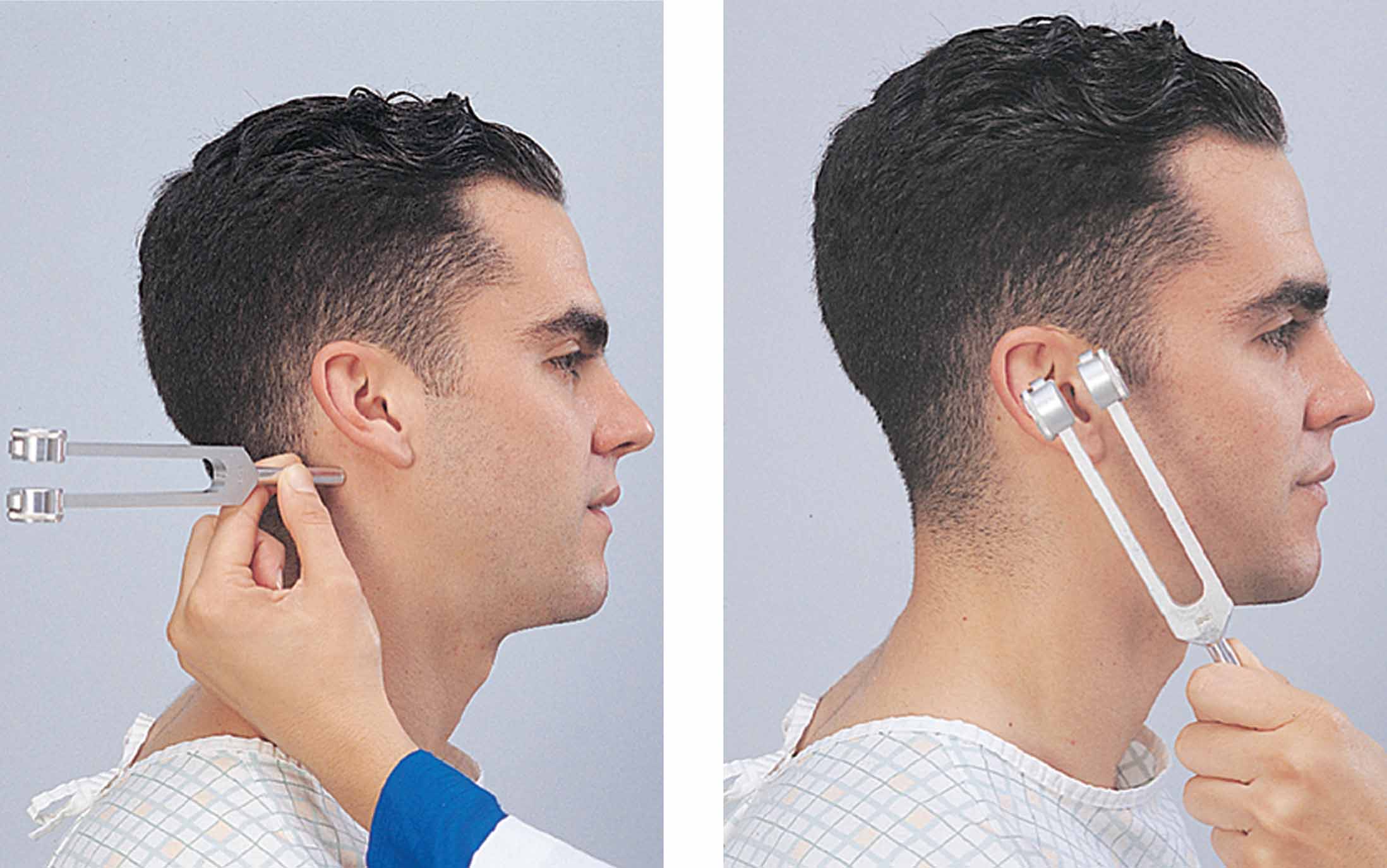
- Weber,
- Rinne,
- Schwabach,
- acoustic emission.
Weber
The technique is used to determine in people who suffer from hearing loss. It allows you to determine the degree of neurosensory or. The study is carried out using a tuning fork. It is activated and applied to various parts of the head.
During the test, a person is asked to listen and answer a question about which ear hears better. A healthy person hears well in both ears. If there is deafness, the sound will be louder in the affected ear. To prevent the ear from adapting to sounds, it is brought up every 4-5 seconds.
Bone conduction testing is carried out using a bass tuning fork. Its leg is placed in the middle of the crown. The branches must oscillate in the frontal plane.
How is the Weber test performed?
Rinne
When conducting such a test, a sounding tuning fork is placed near the platform mastoid process. When the perception of sound stops, the device is brought to the external auditory canal. With a positive experience, there is a predominance air conduction sound over the bone. When negative, it’s the other way around. A positive experience indicates normal hearing.
During the test, the teeth of the tuning fork are set into oscillatory motion in the same way as during the Weber test. The patient is warned that they will hear two sounds: one in the bone behind the ear and one in the ear itself. You need to answer without thinking about which sound is louder.
How to perform the Rinne test
Schwabach
A tuning fork is also placed on the . In case of pathologies, it is revealed that the bone conduction time is reduced or equal to 0. If it is affected, then the bone conduction time increases.
The study is conducted on two subjects. A tuning fork is placed between them. If healthy man hears vibrations, but the patient does not, then further methods Research will be aimed at studying sensorineural hearing loss.
When healthy patient does not hear, but the subject can describe the sounds received, then we are talking about conductive hearing loss.

This method has been used since 1948. It was found that the presence of OAE in people depends on the functioning of the sensitive cells of the hearing organ. If there is sensorineural hearing loss, then there is no otoacoustic emission.
There are two types of UAE:
Detained summoned. It occurs when cochlear cells make oscillatory movements in response to sound received in the form of a broadband sound click. The sound takes a while to reach inner ear and go back in the opposite direction.
Emission at the frequency of the distortion product. It is excited by two pure tones. Since the cochlea has nonlinear properties, in addition to the transmitted tones, distortions appear.
This research is carried out using special equipment. To record the emission, a probe is inserted into the external auditory canal. A small microphone and telephone are built into its body. Research is carried out for each ear separately.
Otoacoustic emissions in newborns

Other methods
In audiometry, audibility is measured in decibels. Thanks to this, the specialist can compare the obtained indicators with the norm. The technique is used for:
- determining sensitivity to sounds,
- air and bone conduction analysis.
The procedure is completely painless and has no contraindications. The patient is given headphones. Through them he receives various signals. The result is an audiogram.
Can be used to assess diseases. It measures the pressure level in the middle ear as well as mobility eardrums. Allows assessment of abnormalities and integrity of the auditory ossicles. The procedure has no contraindications.
Includes the whole complex diagnostic studies, which make it possible to assess the condition auditory tube and middle ear. The peculiarity of the method is that the results do not depend on conditioned reactions.
Can be used for children from an early age. During the conduction process, pressurized air or sound is introduced into the ear canal.
Additionally, electrocochleography may be prescribed. It allows you to evaluate the electrical potentials of the nerve and. Sometimes the method of acoustic brainstem evoked potentials is used to confirm the diagnosis. In this case, the bioelectric reactions of subcortical structures are studied.
How is audiometry performed:
How to check in a child and an adult?
You can test your newborn baby's hearing yourself. If the baby is not yet a month old, then loud noise he may flinch or move his arms. At the age of 2-3 months, the functioning of the auditory organ is simply determined. The baby begins to respond to the mother's voice. The appearance of cooing is the first sign indicating that everything is fine with his hearing.
If you want to test your hearing yourself, then take a squeaky toy, jars with:
- buckwheat,
- peas,
- semolina.
Stand close to the baby. Shake the container with semolina at a distance of 10 cm from the ear. In response to such an action, the child should calm down or show another reaction. After 30 seconds, perform the same procedures with other jars and the toy. The child must react to every action. If there are no changes in behavior, repeat your study after a while.
For adults, the test can be done using a whisper or loud speech. The inspector moves away to a distance of about 6 meters. The subject closes one ear. It is normal if a person heard all the numbers mentioned without any problems.
If spoken phrases are not heard, then the distance between the two subjects decreases. If it is impossible to hear a whisper, a re-test begins with spoken speech.
In conclusion, we note that if due to pathology of the auditory nerve, then its restoration will be almost impossible. Therefore, it is important to carry out timely diagnosis in order to monitor the condition and prevent it from worsening.
Otoacoustic emissions() are low-intensity sounds that are generated by the cochlea and travel through the middle ear into the external auditory canal. Otoacoustic emissions (OAE) are probably not essential for hearing, but are a byproduct active processes, occurring in the outer hair cells.
From a clinical point of view, it is interesting because it is present in normal operation outer hair cells, and is missing if they are damaged. Thus, otoacoustic emission (OAE) determines the consistency of the function of outer hair cells with sufficient accuracy.
There are two types of otoacoustic emissions: spontaneous and evoked. Spontaneous UAE (SOAE) are narrow-band signals that spontaneously arise in the external auditory canal without any stimulus. Spontaneous emission is present in more than half of normal hearing ears and is absent in all ears at frequencies where sensorineural hearing loss exceeds 30 dB. It is believed that OSAE occurs in the outer hair cells corresponding to the portion of the basement membrane that is tuned to this frequency.
For registration spontaneous otoacoustic emissions (SOAE) a highly sensitive microphone placed in an attachment is used with low level noise. The nozzle is secured in the external auditory canal with an elastic cuff. The signals captured by the microphone are sent to a spectrum analyzer, which provides frequency analysis of the signal. Typically, frequencies of interest are detected several times and the results are averaged to remove background noise. OSAE, if it occurs, is manifested by several peaks in the frequency spectrum.
Because of spontaneous otoacoustic emissions (SOAE) is normally absent in many people, it has not found clinical application in practice. Attempts to link OSAE with tinnitus have in some cases found a relationship, but only in small quantity observations, the presence of both SOAE and noise was noted.
Evoked otoacoustic emissions (UAE) is caused by a stimulus and occurs during and after the signal is given. The evoked OAE is similar to the inducing stimulus. There are several types of evoked AOE, two of which have proven clinically useful: stimulation-frequency OAE (TEOAE) and distortion-product frequency OAE (DPOAE).
TEOAE obtained by applying temporary signals or clicks. A series of stimuli - clicks - is usually delivered at intensity levels of 80-85 dB. The signal received from the microphone is averaged, typically over a time window of 20 ms. In the clinical paradigm, alternating emission bursts are placed in separate memory locations so that the final output contains two response traces for comparative purposes.
a - System for recording delayed evoked otoacoustic emissions (LEOAE).A probe with a microphone and loudspeaker is inserted into the external auditory canal.
Acoustic stimuli in the form of clicks are delivered through a loudspeaker and the evoked emission from the cochlea is recorded using a miniature microphone;
b - System for recording otoacoustic emissions at the frequency of the distortion product. The cochlea is stimulated with two tones with frequencies f1 and f2.
Using a microphone, the change in sound pressure in the external auditory canal is recorded along with the primary tones.
The curve in the figure represents the frequency spectrum of the signal recorded by the microphone.
TEOAE occurs approximately 4 ms after the stimulus and lasts approximately 10 ms. Because the click is a broad spectrum signal, its response also has wide range. According to the conditions, these signal forms are subjected to spectral analysis, the results of which are usually presented in the form of a graph reflecting the amplitude-frequency characteristics of the emission. One important aspect TEOAE is the similarity of the answer.
Is it similarity or reproducibility? sequential selection of responses expressed as a percentage, where 100% is taken as identical. The presence of an emission is determined when its volume exceeds the noise volume and the reproducibility is above a specified level. If emission occurs, then it is likely that the external auditory cells function in the emission frequency range.
DPOAE occurs as a result of nonlinear processes in the cochlea. When two tones are applied to the cochlea, distortion occurs in the form of the appearance of other tones that were not present in the two signals supplied. This distortion represents a combination of tones, or harmonics, that correlates with the mathematically predicted tones.
Two tones used to produce DPOAE, according to generally accepted provisions, are designated as f 1 and f 2. The most obvious distortion product occurs at the 2f 1 -f 2 frequency level. As with TEOAE, a special probe is used to deliver the tone pair and record the response. Pairs of tones to obtain the distortion product are applied over the entire frequency range from 1000 to 6000 Hz. Pairs of tones usually have a fixed frequency and relationship regarding intensity.
Typically, pairs are represented by high and low frequencies. After sending a pair of tones to determine otoacoustic emission amplitudes (UAE) at the frequency of the distortion product, the frequency is calculated using the formula, as well as nearby frequencies, to estimate the threshold noise at that point in time.
DPOAE, as a rule, is described as the dependence of the intensity of the distortion product (2f 1 - f 2) on the stimulation frequency (f 2). If the amplitude exceeds the background noise, an emission is said to be present. If emission is present, then most likely the outer hair cells function in the frequency range f 2 tones.
results TEOAE And DPOAE testing allows us to assess the integrity of the function of the outer hair cells. Both approaches have found successful clinical use as an objective indicator of cochlear functioning.
Today, otoacoustic emission is considered one of the most accurate, safe and painless ways testing the perception of auditory information. This method has been successfully used to diagnose hearing in infants.
It is very important to identify hearing loss in a child as early as possible in order to begin treatment for it. early stage. Registration of otoacoustic emissions is a modern and popular technique auditory diagnostics. Thanks to otoacoustic emission recording devices, it is possible to quickly and effectively detect hearing impairment not only in children, but also in adult patients.
What is the essence of otoacoustic emissions?
Using an otoacoustic emission recording apparatus, the doctor can get the most complete picture of the child’s hearing and the state of the structures of his inner ear.
The essence of the method is to obtain an acoustic response, which indicates the normal functioning of the auditory receptor. The device responds to weak sound vibrations generated by the cochlea, which are recorded in the external auditory canal using a highly sensitive microphone.
Types of otoacoustic emissions
IN medical practice There are two types of otoacoustic emissions: evoked and spontaneous. Evoked emission is recorded in response to sound stimulation, while spontaneous emission can be recorded even in the absence of sound signals.
How the research is carried out
To conduct an otoacoustic emissions test, the doctor inserts a special probe into the child's external auditory canal. A miniature microphone and telephone are built into its body. If it is necessary to conduct a study of evoked otoacoustic emissions, broadband signals - clicks - are sent into the ear canal.
The method is automated to the maximum, it allows you to understand whether the baby has hearing problems or not. However, based on the screening results obtained, it is impossible to talk about making an accurate diagnosis.
The study is usually carried out in the maternity hospital 3-4 days after the baby is born. Later the screening is repeated at the age of 1 month. If otoacoustic emissions are not re-identified, the child must be shown to an audiologist for further diagnosis and treatment of the disease.
The phenomenon of otoacoustic emissions is used in medicine to evaluate the functioning of the inner ear. This research technique makes it possible to detect hearing impairment in newborns, but an accurate diagnosis is made only after additional examination.
The audiometer for newborns OtoRead, manufactured by Interacoustics (Denmark) is a the latest system registration of otoacoustic emissions. The small, portable device works quickly, accurately and fully automatically, allowing you to conduct otoacoustic examinations in newborns and obtain the first data on the state of hearing.
Otoacoustic emissions are induced sound produced in the cochlea when it is stimulated by external sound. The absence of evoked otoacoustic emissions may be a sign of certain pathologies of the cochlear apparatus and middle ear. In particular, the diagnosis of hearing loss in newborns necessarily includes the OAE test. OtoRead records the evoked otoacoustic vibrations and stores them in memory. Moreover, both delayed otoacoustic emission (DEOAE) and emission at the frequency of the distortion product (EDF) are supported - you just need to calibrate the device.
The OtoRead system is a convenient probe with interchangeable tips for quick screening, a simple keyboard (only 4 buttons!), a four-line screen and a convenient design that allows you to operate the device with one hand. Choose required test, run the test, view the results - the ergonomics of OtoRead were designed taking into account the opinions of otolaryngologists, and you can get used to the functions of the device within half an hour. The weight of the device is only 300 grams. It works completely autonomously and does not require wires or connection to a computer. Consequently, the doctor has the greatest freedom of action, and small patients do not experience discomfort.
The OtoRead otoacoustic emission registration system model range includes 6 delivery options: Screening+, Screening DP, Screening TE, Standard DP, Standard TE, Standard TE+DP. Models differ in the range of supported frequencies (in the DP modification - up to 12 kHz) and the otoacoustic emission tests performed.
The results of the OAE test are not independent, but in combination with other hearing testing methods, OtoRead will help quickly and accurately diagnose sensorineural hearing loss and various pathologies middle ear. In addition, the system itself is an excellent diagnostic tool for detecting ototoxicity.
The OtoRead audiometer for newborns can be connected to a computer to synchronize with the ENT-Master system. The device itself stores up to 250 measurement results, but it is more convenient to view, filter and analyze screening data on a computer. Moreover, ENT-Master provides the doctor with convenient tools for generating reports and printing examination protocols.